My pain is my prisoner, it's not what I want
It makes me to lie down between hospital sheets
It destroyeth my soul:
It loses me in the paths of sickness, I’m sick of its name Even tho I walk down the hospital corridors is till fear evil,
Tho my drip is with me its pole and its bad don’t comfort me
They prepare others tables in the presence of my nausea
They assault my body with drugs, my patience runs out.
Surely illness and despair will leave me and I will dwell in this house of sickness no MORE!!
This was posted on the PMB with a request to find out who the orginal Author was. So if you can help then please feel free to post a comment. Thanks for your help.
Tuesday, August 22, 2006
Wednesday, August 02, 2006
What does S.O.D. Stand for?
In Reply to: ps. what does sod stand for? posted by jeff on July 24, 2006 at
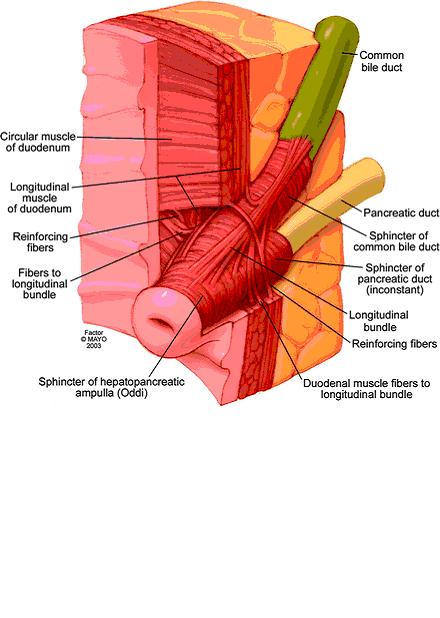
Sphincter of oddi disfunction.. its also on jerrys blog.. I'll put the pic here and then paste the info in this post**************************************************
This is a picture that shows the sphincter of oddi. the main pancreatic duct and bile duct from the liver both converge and their liquids are released via the sphincter. The main pancreatic duct will back up with activated enzymes and they will eat and destroy all along the length of the pancreas. In the torso diagram, where the head of the pancreas is (torsos right side) Jerry has a knot that protrudes out of his abdomen. We were todl that the pancreas is swelling so large that it pushes out from under the stomach and that is what is causing the bulge.*******************************************
ps the bulge is gone and has not returned! so it was the pancreas and NOT a food bolus!
Insurance Help Sites
Posted by cj on July 10, 2006 at 14:49:28:In Reply to: no insurance and help?
Patient assistance programs-helpingpatients.org/
--------------------------------------------------------------------------------
www.togetherrxaccess.com/
www.medicare.gov
www.disabilityresources.org To find disability organizations or agenices in your area, click on your home state:
http://www.ncpad.org/organizations/alpha
http://www.focusas.com/HealthInfoNumbers.htm Toll-Free Numbers for Health Information
http://www.3m.com/us/healthcare/pha...ssistance.jhtml
http://sis.nlm.nih.gov/hotlines/
http://coveringkidsandfamilies.org/communications/bts/
http://www.freemedicineprogram.com/drug/ELDER+TONIC/
http://www.mycancernews.com/viatical.html
http://www.cancercare.org/HelpingHa...deList.cfm?c=49
http://www.helpingpatients.org/
http://www.rxassist.org/default.cfm
http://www.doctorhealthynet.com/fre...dicine_home.htm
http://www.needymeds.com/
http://www.mhsanctuary.com/add/rx.htm
http://www.astrazeneca-us.com/content/drugAssistance/
https://www.merck.com/pap/pap/consu...application.jsp
http://www.pfizer.com/subsites/phil...ents.index.html
http://www.sch-plough.com/schering_...nt_programs.jsp
http://www.phrma.org/
http://www.hrsa.gov/osp/dfcr/obtain/obtain.htm
http://www.lillyanswers.com/
http://www.benefitscheckup.com/
http://www.pharma.us.novartis.com/i...?TNav&checked=y
Patient assistance programs-helpingpatients.org/
--------------------------------------------------------------------------------
www.togetherrxaccess.com/
www.medicare.gov
www.disabilityresources.org To find disability organizations or agenices in your area, click on your home state:
http://www.ncpad.org/organizations/alpha
http://www.focusas.com/HealthInfoNumbers.htm Toll-Free Numbers for Health Information
http://www.3m.com/us/healthcare/pha...ssistance.jhtml
http://sis.nlm.nih.gov/hotlines/
http://coveringkidsandfamilies.org/communications/bts/
http://www.freemedicineprogram.com/drug/ELDER+TONIC/
http://www.mycancernews.com/viatical.html
http://www.cancercare.org/HelpingHa...deList.cfm?c=49
http://www.helpingpatients.org/
http://www.rxassist.org/default.cfm
http://www.doctorhealthynet.com/fre...dicine_home.htm
http://www.needymeds.com/
http://www.mhsanctuary.com/add/rx.htm
http://www.astrazeneca-us.com/content/drugAssistance/
https://www.merck.com/pap/pap/consu...application.jsp
http://www.pfizer.com/subsites/phil...ents.index.html
http://www.sch-plough.com/schering_...nt_programs.jsp
http://www.phrma.org/
http://www.hrsa.gov/osp/dfcr/obtain/obtain.htm
http://www.lillyanswers.com/
http://www.benefitscheckup.com/
http://www.pharma.us.novartis.com/i...?TNav&checked=y
Bristol Stool Scale
Bristol Stool ScaleFrom Wikipedia, the free encyclopediaYou have new messages (last change).Jump to: navigation, search
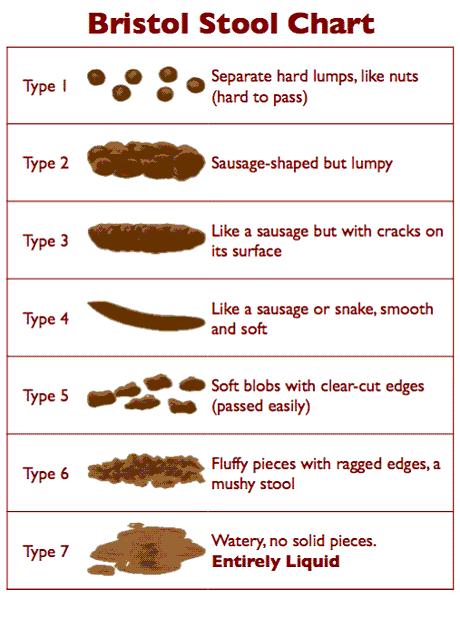
The Bristol Stool Scale or Bristol Stool Chart is a medical aid designed to classify the faeces form into seven groups. It was developed by Heaton and Lewis at the University of Bristol and was first published in the journal Scand J Gastroenterol in 1997. Because the form of the stool depends on the time it spends in the colon, there is a correlation between the colonic transit time and the stool type.
The seven types of stool are:
Type 1: Separate hard lumps, like nuts (hard to pass)
Type 2: Sausage-shaped, but lumpy
Type 3: Like a sausage but with cracks on its surface
Type 4: Like a sausage or snake, smooth and soft
Type 5: Soft blobs with clear cut edges (passed easily)
Type 6: Fluffy pieces with ragged edges, a mushy stool
Type 7: Watery, no solid pieces (entirely liquid)
Types 1 and 2 indicate constipation, with 3 and 4 being the "ideal stools" especially the latter, as they are the easiest to pass. 5-7 being further tending towards diarrhoea.
[edit]ReferencesConstipation Management and Nurse Prescribing: The importance of developing a concordant approach PDF Faecal incontinence and constipation PDF [edit]External linksThe Bristol Stool Scale from Medscape.com Information from Solvay Pharmaceuticals Childhood Constipation Retrieved from "http://en.wikipedia.org/wiki/Bristol_Stool_Scale"Categories: General practice | Gastroenterology
Ambry Test
Posted by cj on July 20, 2006 at 16:10:14
http://www.ambrygen.com/reports/Pancreatitis%20Sales%20Aid%205-06.pdf
The Ambry Test : PancreatitisPancreatitis is a serious problem with asignificant genetic component.Pancreatitis accounts for 87,000 hospitalizationsper year in the US.1 Chronic pancreatitis patientsface a 26-fold increased risk of pancreatic cancer,and for those with hereditary pancreatitis, the riskis 50-fold with approximately 40% developingpancreatic cancer by age 70.2Normal exocrine pancreatic function depends on adelicate balance of enzyme activation andinhibition which can be affected by multipleenvironmental and genetic factors. Hereditarypancreatitis has been linked to mutations in thePRSS1 gene. Study of idiopathic chronic andrecurrent acute pancreatitis demonstrates thatmutations in three genes – PRSS1, SPINK1, andCFTR – predispose to pancreatitis.3Due to the cumulative contribution of three genesin both dominant and recessive patterns, a patientmay have genetically-determined pancreatitis evenif family history is negative.Ambry Genetics offers the world’s onlycomprehensive genetic test for pancreatitis.To help determine etiology and suggestappropriate treatments, Ambry Genetics offersanalysis of all coding regions of the CFTR, PRSS1,and SPINK1 genes in The Ambry Test: PancreatitisAMPLIFIED™. This test also analyzes the CFTRgene for gross deletions and duplications, whenindicated, providing a detection rate ofapproximately 99% for each gene. The panel isalso available without CFTR deletion/duplicationanalysis (The Ambry Test: Pancreatitis, CFdetection rate 97-98%), and each test is availableseparately.100 Columbia #200 | Aliso Viejo, CA 92656 | 949 900 5500fax 949 900 5501 | toll free 866 262 7943 |
www.ambrygen.com|
Pancreatitis1 in 4 patients tests positive for at least onesignificant genetic mutation.Mutations in three genes predispose to chronicand recurrent acute pancreatitis:• CFTR – cystic fibrosis transmembraneconductance regulator• PRSS1 – cationic trypsinogen• SPINK1 – serine protease inbitor, Kazal type 1Genetic testing for pancreatitis can help you:• Avoid repeated diagnostic testing• Provide targeted therapy• Address increased cancer risk in geneticallydeterminedpancreatitis• Help your patient understand his condition andincrease compliance• Communicate inheritance risks tofamily membersNo other test can identifymore mutations thanThe Ambry Test:Pancreatitis AMPLIFIEDGet started with Ambry Genetics today.Sample submission kits are available atno charge. Please call 866-262-7943 or visitour website to obtain more information andall necessary forms.™100 Columbia #200 | Aliso Viejo, CA 92656 | 949 900 5500fax 949 900 5501 | toll free 866 262 7943 | www.ambrygen.com|
Pancreatitis• In the entire patient set, 49.1% (116/236) carriedat least one mutation.• 11.0% (26/236) had a form of CF confirmed by2 CF mutations. An additional 22.0% (52/236)had one CF mutation.• 8.9% (21/236) had mutations in more than one gene.• Only 4.2% (10/236) patients had PRSS1mutations only.• Approximately 1/4 patients (23.7%, 56/256) havemutations with a clear causative component(defined as presence of 2 CF mutations and/orknown deleterious PRSS1 or SPINK1 mutations).83891, 83894, 83898,83903, 83904, 83909,839123-5 WeeksFull gene mutation scanning is performed by modified TemporalTemperature Gradient Electrophoresis (mTTGE). All sequencevariations detected by mTTGE are identified by double-strandedautomated sequencing. If indicated, CFTR gross deletion /duplication testing is performed by MLPA (MRC Holland).Blood: 5cc peripheral blood in purple-top EDTA (preferred) oryellow top ACD. Store at 2-8° C up to 96 hours prior toshipping. Do not freeze. Ship at room temperature.CPT CodesTurn-Around-TimeMethodSpecimenRequirements1 Yakshe P. Pancreatitis, chronic. emedicine [online resource]. Available at: http://www.emedicine.com/MED/topic1721.htm. Last update July 2005.2 Erickson RA. Pancreatic cancer. emedicine [online resource]. Available at: http://www.emedicine.com/MED/topic1712.htm. Last update Dec 2005.3 Etemad B, Whitcomb DC. Gastroenterology. 2001;120:682-707.4 Whitcomb DC.US Gastro Review. 2006;56-58, and personal communication.© 2006 Ambry Genetics. All rights reserved. P0506-09-003-MKG-00.PANCREATITIS PANEL PANCREATITIS PANEL AMPLIFIED83891, 83894, 83898, 83900,83901, 83903, 83904, 83909,839124-6 Weeks1 in 4 patients has at least onesignificant mutation.In a series of patients with chronic or recurrentacute pancreatitis, The Ambry Test: Pancreatitisdetected at least one mutation in 49.1% (116/236).Though patients known to have cystic fibrosis (CF)were excluded from this series, 11.0% (26/236) werefound to have a form of CF confirmed with at leasttwo CFTR mutations. Nearly as many patients(8.9%, 21/236) had mutations in more thanone gene.Using a stricter definition of clinical significance aspresence of known deleterious mutations in PRSS1or SPINK1, and/or two CF mutations, approximatelyone in four patients (23.7%, 56/236) has a causativegenetic component to their pancreatitis.Genetic testing results can help youmanage your patient.As mutations in different genes affect differentsteps of trypsin activation and inhibition, genetictesting can suggest treatments targeted to apatient’s particular defect. For example, PRSS1mutations may lead to premature trypsinogenactivation through altered sensitivity to calcium.Preventive measures could include various steps tominimize stimulation of the acinar cells and assistcalcium regulation.4 CFTR mutations impairpancreatic duct flushing, so treatments could focuson stimulating the pancreas and maximizing flowthrough the duct.4Identifying patients with mutations allowsappropriately increased cancer surveillance.Knowledge of contributory mutations explains thedisease to the patient, reinforces understanding ofits chronic nature, and affirms the importance ofcompliance with dietary and lifestyle modifications.Further, family members may be tested andcounseled to minimize their risk of developingchronic pancreatitis.Mutation distribution in 236 patients testedwith The Ambry Test: Pancreatitits
The Ambry Test : PancreatitisPancreatitis is a serious problem with asignificant genetic component.Pancreatitis accounts for 87,000 hospitalizationsper year in the US.1 Chronic pancreatitis patientsface a 26-fold increased risk of pancreatic cancer,and for those with hereditary pancreatitis, the riskis 50-fold with approximately 40% developingpancreatic cancer by age 70.2Normal exocrine pancreatic function depends on adelicate balance of enzyme activation andinhibition which can be affected by multipleenvironmental and genetic factors. Hereditarypancreatitis has been linked to mutations in thePRSS1 gene. Study of idiopathic chronic andrecurrent acute pancreatitis demonstrates thatmutations in three genes – PRSS1, SPINK1, andCFTR – predispose to pancreatitis.3Due to the cumulative contribution of three genesin both dominant and recessive patterns, a patientmay have genetically-determined pancreatitis evenif family history is negative.Ambry Genetics offers the world’s onlycomprehensive genetic test for pancreatitis.To help determine etiology and suggestappropriate treatments, Ambry Genetics offersanalysis of all coding regions of the CFTR, PRSS1,and SPINK1 genes in The Ambry Test: PancreatitisAMPLIFIED™. This test also analyzes the CFTRgene for gross deletions and duplications, whenindicated, providing a detection rate ofapproximately 99% for each gene. The panel isalso available without CFTR deletion/duplicationanalysis (The Ambry Test: Pancreatitis, CFdetection rate 97-98%), and each test is availableseparately.100 Columbia #200 | Aliso Viejo, CA 92656 | 949 900 5500fax 949 900 5501 | toll free 866 262 7943 | www.ambrygen.com| Pancreatitis
1 in 4 patients tests positive for at least onesignificant genetic mutation.Mutations in three genes predispose to chronicand recurrent acute pancreatitis:• CFTR – cystic fibrosis transmembraneconductance regulator• PRSS1 – cationic trypsinogen• SPINK1 – serine protease inbitor, Kazal type 1Genetic testing for pancreatitis can help you:• Avoid repeated diagnostic testing• Provide targeted therapy• Address increased cancer risk in geneticallydeterminedpancreatitis• Help your patient understand his condition andincrease compliance• Communicate inheritance risks tofamily membersNo other test can identifymore mutations thanThe Ambry Test:Pancreatitis AMPLIFIEDGet started with Ambry Genetics today.Sample submission kits are available atno charge. Please call 866-262-7943 or visitour website to obtain more information andall necessary forms.™100 Columbia #200 | Aliso Viejo, CA 92656 | 949 900 5500fax 949 900 5501 | toll free 866 262 7943 | www.ambrygen.com| Pancreatitis•
In the entire patient set, 49.1% (116/236) carriedat least one mutation.• 11.0% (26/236) had a form of CF confirmed by2 CF mutations. An additional 22.0% (52/236)had one CF mutation.• 8.9% (21/236) had mutations in more than one gene.• Only 4.2% (10/236) patients had PRSS1mutations only.• Approximately 1/4 patients (23.7%, 56/256) havemutations with a clear causative component(defined as presence of 2 CF mutations and/orknown deleterious PRSS1 or SPINK1 mutations).83891, 83894, 83898,83903, 83904, 83909,839123-5 WeeksFull gene mutation scanning is performed by modified TemporalTemperature Gradient Electrophoresis (mTTGE). All sequencevariations detected by mTTGE are identified by double-strandedautomated sequencing. If indicated, CFTR gross deletion /duplication testing is performed by MLPA (MRC Holland).Blood: 5cc peripheral blood in purple-top EDTA (preferred) oryellow top ACD. Store at 2-8° C up to 96 hours prior toshipping. Do not freeze. Ship at room temperature.CPT CodesTurn-Around-TimeMethodSpecimenRequirements1 Yakshe P. Pancreatitis, chronic. emedicine [online resource]. Available at: http://www.emedicine.com/MED/topic1721.htm. Last update July 2005.2 Erickson RA. Pancreatic cancer. emedicine [online resource]. Available at: http://www.emedicine.com/MED/topic1712.htm. Last update Dec 2005.3 Etemad B, Whitcomb DC. Gastroenterology. 2001;120:682-707.4 Whitcomb DC.US Gastro Review. 2006;56-58, and personal communication.© 2006 Ambry Genetics. All rights reserved. P0506-09-003-MKG-00.PANCREATITIS PANEL PANCREATITIS PANEL AMPLIFIED83891, 83894, 83898, 83900,83901, 83903, 83904, 83909,839124-6 Weeks
1 in 4 patients has at least onesignificant mutation.In a series of patients with chronic or recurrentacute pancreatitis, The Ambry Test: Pancreatitisdetected at least one mutation in 49.1% (116/236).Though patients known to have cystic fibrosis (CF)were excluded from this series, 11.0% (26/236) werefound to have a form of CF confirmed with at leasttwo CFTR mutations. Nearly as many patients(8.9%, 21/236) had mutations in more thanone gene.Using a stricter definition of clinical significance aspresence of known deleterious mutations in PRSS1or SPINK1, and/or two CF mutations, approximatelyone in four patients (23.7%, 56/236) has a causativegenetic component to their pancreatitis.Genetic testing results can help youmanage your patient.As mutations in different genes affect differentsteps of trypsin activation and inhibition, genetictesting can suggest treatments targeted to apatient’s particular defect. For example, PRSS1mutations may lead to premature trypsinogenactivation through altered sensitivity to calcium.Preventive measures could include various steps tominimize stimulation of the acinar cells and assistcalcium regulation.4 CFTR mutations impairpancreatic duct flushing, so treatments could focuson stimulating the pancreas and maximizing flowthrough the duct.4Identifying patients with mutations allowsappropriately increased cancer surveillance.Knowledge of contributory mutations explains thedisease to the patient, reinforces understanding ofits chronic nature, and affirms the importance ofcompliance with dietary and lifestyle modifications.Further, family members may be tested andcounseled to minimize their risk of developingchronic pancreatitis.Mutation distribution in 236 patients testedwith The Ambry Test: Pancreatitits
http://www.ambrygen.com/reports/Pancreatitis%20Sales%20Aid%205-06.pdf
The Ambry Test : PancreatitisPancreatitis is a serious problem with asignificant genetic component.Pancreatitis accounts for 87,000 hospitalizationsper year in the US.1 Chronic pancreatitis patientsface a 26-fold increased risk of pancreatic cancer,and for those with hereditary pancreatitis, the riskis 50-fold with approximately 40% developingpancreatic cancer by age 70.2Normal exocrine pancreatic function depends on adelicate balance of enzyme activation andinhibition which can be affected by multipleenvironmental and genetic factors. Hereditarypancreatitis has been linked to mutations in thePRSS1 gene. Study of idiopathic chronic andrecurrent acute pancreatitis demonstrates thatmutations in three genes – PRSS1, SPINK1, andCFTR – predispose to pancreatitis.3Due to the cumulative contribution of three genesin both dominant and recessive patterns, a patientmay have genetically-determined pancreatitis evenif family history is negative.Ambry Genetics offers the world’s onlycomprehensive genetic test for pancreatitis.To help determine etiology and suggestappropriate treatments, Ambry Genetics offersanalysis of all coding regions of the CFTR, PRSS1,and SPINK1 genes in The Ambry Test: PancreatitisAMPLIFIED™. This test also analyzes the CFTRgene for gross deletions and duplications, whenindicated, providing a detection rate ofapproximately 99% for each gene. The panel isalso available without CFTR deletion/duplicationanalysis (The Ambry Test: Pancreatitis, CFdetection rate 97-98%), and each test is availableseparately.100 Columbia #200 | Aliso Viejo, CA 92656 | 949 900 5500fax 949 900 5501 | toll free 866 262 7943 |
www.ambrygen.com|
Pancreatitis1 in 4 patients tests positive for at least onesignificant genetic mutation.Mutations in three genes predispose to chronicand recurrent acute pancreatitis:• CFTR – cystic fibrosis transmembraneconductance regulator• PRSS1 – cationic trypsinogen• SPINK1 – serine protease inbitor, Kazal type 1Genetic testing for pancreatitis can help you:• Avoid repeated diagnostic testing• Provide targeted therapy• Address increased cancer risk in geneticallydeterminedpancreatitis• Help your patient understand his condition andincrease compliance• Communicate inheritance risks tofamily membersNo other test can identifymore mutations thanThe Ambry Test:Pancreatitis AMPLIFIEDGet started with Ambry Genetics today.Sample submission kits are available atno charge. Please call 866-262-7943 or visitour website to obtain more information andall necessary forms.™100 Columbia #200 | Aliso Viejo, CA 92656 | 949 900 5500fax 949 900 5501 | toll free 866 262 7943 | www.ambrygen.com|
Pancreatitis• In the entire patient set, 49.1% (116/236) carriedat least one mutation.• 11.0% (26/236) had a form of CF confirmed by2 CF mutations. An additional 22.0% (52/236)had one CF mutation.• 8.9% (21/236) had mutations in more than one gene.• Only 4.2% (10/236) patients had PRSS1mutations only.• Approximately 1/4 patients (23.7%, 56/256) havemutations with a clear causative component(defined as presence of 2 CF mutations and/orknown deleterious PRSS1 or SPINK1 mutations).83891, 83894, 83898,83903, 83904, 83909,839123-5 WeeksFull gene mutation scanning is performed by modified TemporalTemperature Gradient Electrophoresis (mTTGE). All sequencevariations detected by mTTGE are identified by double-strandedautomated sequencing. If indicated, CFTR gross deletion /duplication testing is performed by MLPA (MRC Holland).Blood: 5cc peripheral blood in purple-top EDTA (preferred) oryellow top ACD. Store at 2-8° C up to 96 hours prior toshipping. Do not freeze. Ship at room temperature.CPT CodesTurn-Around-TimeMethodSpecimenRequirements1 Yakshe P. Pancreatitis, chronic. emedicine [online resource]. Available at: http://www.emedicine.com/MED/topic1721.htm. Last update July 2005.2 Erickson RA. Pancreatic cancer. emedicine [online resource]. Available at: http://www.emedicine.com/MED/topic1712.htm. Last update Dec 2005.3 Etemad B, Whitcomb DC. Gastroenterology. 2001;120:682-707.4 Whitcomb DC.US Gastro Review. 2006;56-58, and personal communication.© 2006 Ambry Genetics. All rights reserved. P0506-09-003-MKG-00.PANCREATITIS PANEL PANCREATITIS PANEL AMPLIFIED83891, 83894, 83898, 83900,83901, 83903, 83904, 83909,839124-6 Weeks1 in 4 patients has at least onesignificant mutation.In a series of patients with chronic or recurrentacute pancreatitis, The Ambry Test: Pancreatitisdetected at least one mutation in 49.1% (116/236).Though patients known to have cystic fibrosis (CF)were excluded from this series, 11.0% (26/236) werefound to have a form of CF confirmed with at leasttwo CFTR mutations. Nearly as many patients(8.9%, 21/236) had mutations in more thanone gene.Using a stricter definition of clinical significance aspresence of known deleterious mutations in PRSS1or SPINK1, and/or two CF mutations, approximatelyone in four patients (23.7%, 56/236) has a causativegenetic component to their pancreatitis.Genetic testing results can help youmanage your patient.As mutations in different genes affect differentsteps of trypsin activation and inhibition, genetictesting can suggest treatments targeted to apatient’s particular defect. For example, PRSS1mutations may lead to premature trypsinogenactivation through altered sensitivity to calcium.Preventive measures could include various steps tominimize stimulation of the acinar cells and assistcalcium regulation.4 CFTR mutations impairpancreatic duct flushing, so treatments could focuson stimulating the pancreas and maximizing flowthrough the duct.4Identifying patients with mutations allowsappropriately increased cancer surveillance.Knowledge of contributory mutations explains thedisease to the patient, reinforces understanding ofits chronic nature, and affirms the importance ofcompliance with dietary and lifestyle modifications.Further, family members may be tested andcounseled to minimize their risk of developingchronic pancreatitis.Mutation distribution in 236 patients testedwith The Ambry Test: Pancreatitits
The Ambry Test : PancreatitisPancreatitis is a serious problem with asignificant genetic component.Pancreatitis accounts for 87,000 hospitalizationsper year in the US.1 Chronic pancreatitis patientsface a 26-fold increased risk of pancreatic cancer,and for those with hereditary pancreatitis, the riskis 50-fold with approximately 40% developingpancreatic cancer by age 70.2Normal exocrine pancreatic function depends on adelicate balance of enzyme activation andinhibition which can be affected by multipleenvironmental and genetic factors. Hereditarypancreatitis has been linked to mutations in thePRSS1 gene. Study of idiopathic chronic andrecurrent acute pancreatitis demonstrates thatmutations in three genes – PRSS1, SPINK1, andCFTR – predispose to pancreatitis.3Due to the cumulative contribution of three genesin both dominant and recessive patterns, a patientmay have genetically-determined pancreatitis evenif family history is negative.Ambry Genetics offers the world’s onlycomprehensive genetic test for pancreatitis.To help determine etiology and suggestappropriate treatments, Ambry Genetics offersanalysis of all coding regions of the CFTR, PRSS1,and SPINK1 genes in The Ambry Test: PancreatitisAMPLIFIED™. This test also analyzes the CFTRgene for gross deletions and duplications, whenindicated, providing a detection rate ofapproximately 99% for each gene. The panel isalso available without CFTR deletion/duplicationanalysis (The Ambry Test: Pancreatitis, CFdetection rate 97-98%), and each test is availableseparately.100 Columbia #200 | Aliso Viejo, CA 92656 | 949 900 5500fax 949 900 5501 | toll free 866 262 7943 | www.ambrygen.com| Pancreatitis
1 in 4 patients tests positive for at least onesignificant genetic mutation.Mutations in three genes predispose to chronicand recurrent acute pancreatitis:• CFTR – cystic fibrosis transmembraneconductance regulator• PRSS1 – cationic trypsinogen• SPINK1 – serine protease inbitor, Kazal type 1Genetic testing for pancreatitis can help you:• Avoid repeated diagnostic testing• Provide targeted therapy• Address increased cancer risk in geneticallydeterminedpancreatitis• Help your patient understand his condition andincrease compliance• Communicate inheritance risks tofamily membersNo other test can identifymore mutations thanThe Ambry Test:Pancreatitis AMPLIFIEDGet started with Ambry Genetics today.Sample submission kits are available atno charge. Please call 866-262-7943 or visitour website to obtain more information andall necessary forms.™100 Columbia #200 | Aliso Viejo, CA 92656 | 949 900 5500fax 949 900 5501 | toll free 866 262 7943 | www.ambrygen.com| Pancreatitis•
In the entire patient set, 49.1% (116/236) carriedat least one mutation.• 11.0% (26/236) had a form of CF confirmed by2 CF mutations. An additional 22.0% (52/236)had one CF mutation.• 8.9% (21/236) had mutations in more than one gene.• Only 4.2% (10/236) patients had PRSS1mutations only.• Approximately 1/4 patients (23.7%, 56/256) havemutations with a clear causative component(defined as presence of 2 CF mutations and/orknown deleterious PRSS1 or SPINK1 mutations).83891, 83894, 83898,83903, 83904, 83909,839123-5 WeeksFull gene mutation scanning is performed by modified TemporalTemperature Gradient Electrophoresis (mTTGE). All sequencevariations detected by mTTGE are identified by double-strandedautomated sequencing. If indicated, CFTR gross deletion /duplication testing is performed by MLPA (MRC Holland).Blood: 5cc peripheral blood in purple-top EDTA (preferred) oryellow top ACD. Store at 2-8° C up to 96 hours prior toshipping. Do not freeze. Ship at room temperature.CPT CodesTurn-Around-TimeMethodSpecimenRequirements1 Yakshe P. Pancreatitis, chronic. emedicine [online resource]. Available at: http://www.emedicine.com/MED/topic1721.htm. Last update July 2005.2 Erickson RA. Pancreatic cancer. emedicine [online resource]. Available at: http://www.emedicine.com/MED/topic1712.htm. Last update Dec 2005.3 Etemad B, Whitcomb DC. Gastroenterology. 2001;120:682-707.4 Whitcomb DC.US Gastro Review. 2006;56-58, and personal communication.© 2006 Ambry Genetics. All rights reserved. P0506-09-003-MKG-00.PANCREATITIS PANEL PANCREATITIS PANEL AMPLIFIED83891, 83894, 83898, 83900,83901, 83903, 83904, 83909,839124-6 Weeks
1 in 4 patients has at least onesignificant mutation.In a series of patients with chronic or recurrentacute pancreatitis, The Ambry Test: Pancreatitisdetected at least one mutation in 49.1% (116/236).Though patients known to have cystic fibrosis (CF)were excluded from this series, 11.0% (26/236) werefound to have a form of CF confirmed with at leasttwo CFTR mutations. Nearly as many patients(8.9%, 21/236) had mutations in more thanone gene.Using a stricter definition of clinical significance aspresence of known deleterious mutations in PRSS1or SPINK1, and/or two CF mutations, approximatelyone in four patients (23.7%, 56/236) has a causativegenetic component to their pancreatitis.Genetic testing results can help youmanage your patient.As mutations in different genes affect differentsteps of trypsin activation and inhibition, genetictesting can suggest treatments targeted to apatient’s particular defect. For example, PRSS1mutations may lead to premature trypsinogenactivation through altered sensitivity to calcium.Preventive measures could include various steps tominimize stimulation of the acinar cells and assistcalcium regulation.4 CFTR mutations impairpancreatic duct flushing, so treatments could focuson stimulating the pancreas and maximizing flowthrough the duct.4Identifying patients with mutations allowsappropriately increased cancer surveillance.Knowledge of contributory mutations explains thedisease to the patient, reinforces understanding ofits chronic nature, and affirms the importance ofcompliance with dietary and lifestyle modifications.Further, family members may be tested andcounseled to minimize their risk of developingchronic pancreatitis.Mutation distribution in 236 patients testedwith The Ambry Test: Pancreatitits
Celiac Plexus Block
In Reply to: Celiac Plexus Nerve Blocks posted by Robin H. on August 01, 2006 at 10:42:48:
(image placeholder)
I knew someone on here had had something diff done. Thats why i told jeff, someone else will pipe up with info. also i found this neat page!!
*****************************************************ROUND TABLE
Article in PDF format - JOP Home page
JOP. J Pancreas (Online) 2004; 5(4):315-321.
Celiac Plexus Neurolysis
Paolo Giorgio Arcidiacono, Marzia Rossi
Diagnostic and Therapeutic Endosonography Unit, Division of Gastroenterology and Gastrointestinal Endoscopy, Vita-Salute San Raffaele University - San Raffaele Hospital. Milan, Italy
Introduction
Pancreatic cancer is the tenth most common malignancy and the fourth cause of cancer-related death in Western countries. Because 5-year survival in referral centers is less than 30%, clinical management of most patients involves palliation of the symptoms of which 90% are weight loss, jaundice, and pain.
While jaundice related to biliary obstruction can be palliated by means of endoscopic therapy or surgery, pancreatic pain is often difficult to control.
Initial therapy with non-steroid anti-inflammatory agents (NSAIDs) is often rapidly overwhelmed by pain and necessitates being associated with opioid administration.
Although opioids effectively relieve pain, they are associated with many different collateral effects, such as dry mouth, constipation, nausea, vomiting, drowsiness and delirium, which can determine a great decrease in quality of life and may also impair the immune function. Pancreatic pain is also quite common in patients with chronic pancreatitis and, in this case, pain has a multi-factorial etiology; for this reason, prolonged drug therapy is related to an increased risk of narcotic-dependence [1].
Celiac plexus neurolysis (CPN) is a chemical splanchnicectomy of the celiac plexus; its goal is to ablate the efferent nerve fibres which transmit pain from the intra-abdominal viscera.
Although the terms "celiac plexus" and "splanchnic nerves" are often used interchangeably, these are anatomically distinct structures.
The splanchnic nerves are located above the diaphragm (retro-crural) and are typically anterior to the 12th thoracic vertebra; on the other hand, the celiac plexus is situated below the diaphragm (ante-crural), surrounding the basis of the celiac trunk. This plexus is composed of a dense network of ganglia and interconnecting fibres (Figure 1).
Figure 1. The celiac plexus.
The ganglia vary in number (1-5), size (diameter 0.5-4.5 cm), and location (T12-L2), but, independently on their size, the ganglia cannot be visualized as distinct structures by any kind of imaging modality.
The celiac plexus transmits pain sensation originating from the pancreas and most of the abdominal viscera except for the left colon, rectum and pelvic organs.
Stimuli reach the thalamus and the cortex of the brain, leading to pain sensation. On the contrary, some descending inhibitory mechanisms may also modulate the ascending pain information.
The CPN technique was first described by Kappis et al. in 1919 [2]; since then, a number of modifications have been proposed and introduced in a clinical setting in an attempt to improve the accuracy of needle placement and pain relief while reducing procedure-related complications.
Nowadays, CPN is most commonly used to palliate patients suffering from pain due to pancreatic cancer and chronic pancreatitis; it can be performed using different approaches either percutaneously, surgically or under EUS guidance. Until the 1990s, the most common of the above was surely the percutaneous route, injecting absolute alcohol into the celiac plexus under fluoroscopy or CT guidance.
Different studies have reported data on safety, accuracy in reaching the right site of injection and efficacy in decreasing pain due to different diseases by means of CT-guided CPN.
Some authors described 28 cases of CPN performed under CT guidance in patients having neoplasms originating in the pancreas (n=10), stomach (n=8), bile ducts (n=5), liver (n=3), right colon (n=1) and kidney (n=1) [3]. The study showed that this procedure is safe and efficient in controlling pain [3].
Unfortunately, the CT CPN approach is usually posterior and, for this reason, cases of paraplegia have been reported caused by the puncture of the nervous radix at the time of the introduction of the needle during the procedure [4].
Endoscopic ultrasonography (EUS) is a relatively new imaging technique which couples a high frequency ultrasound probe with an oblique viewing endoscopic instrument. This combination allows the endoscopist to obtain a perfect evaluation of the pancreatic parenchyma and surrounding structures, not least, the aorta and celiac trunk. This imaging modality has achieved wide acceptance as the technique of choice for the evaluation of pancreatic disease, diagnosis and staging of pancreatic cancer, diagnosis of idiopathic pancreatitis and the evidencing of neuro-endocrine neoplasms.
At the beginning of EUS, instruments were provided by radial scanning probes; this means that the scanning plane of these probes was transversal, that is, perpendicular to the longitudinal axis of the endoscopic instrument.
This probe orientation absolutely limited the possibility of these instruments performing EUS guided diagnostic or therapeutic procedures, due to the inability of the probe to follow, under real time guidance, the route of a needle device from the orifice of the working channel of the EUS instrument to a target lesion located either inside the gut wall or, as for CPN, outside the gut wall. In early 1990s, there was a technical revolution in EUS instrumentation; in fact, a longitudinal echoendoscope was presented.
This instrument was made with an electronic convex high frequency probe having a longitudinal scanning plane; this means that the scanning plane was on the same longitudinal axis as the endoscope and, more importantly, on the same axis of the working channel.
This innovation has opened the field of operative EUS, allowing the possibility of following, under real time guidance, any kind of device passed throughout the working channel to reach a target lesion.
Since that time, EUS has been tested in this new operative setting for many reasons, mainly the cytological analysis of tumors and, more recently, it has been applied in the treatment of pain in patients with chronic pancreatitis or pancreatic cancer by injecting neurolytic agents in the area of the celiac plexus.
Although many studies demonstrate that celiac plexus neurolysis effectively controls pancreatic cancer pain, up to 1% of patients undergoing percutaneous CPN may develop serious complications, including lower extremity weakness, paresthesias, including epidural anesthesia, lumbar puncture and pneumothorax.
In theory, EUS CPN is safer than posterior percutaneous techniques because EUS allows direct access to the celiac plexus without risk to the vital spinal nerves, the diaphragm or the spinal arteries.
Procedure
EUS-guided celiac plexus neurolysis (EUS CPN) is usually combined with the biopsy of a pancreatic primary lesion for diagnostic and staging purposes. It is performed with a linear array echoendoscope (Figure 2).
Figure 2. Linear array echoendoscope.
With these instruments, it is possible to follow, under EUS real time guidance, the route of the needle through the pancreatic lesion.
Informed consent is obtained with specific attention to complications associated with CPN and EUS guided fine needle aspiration (FNA) of pancreatic lesions. The procedure is performed under deep sedation under the supervision of an anesthesiologist. The patient lays on left lateral decubitus and his/her vital parameters are monitored.
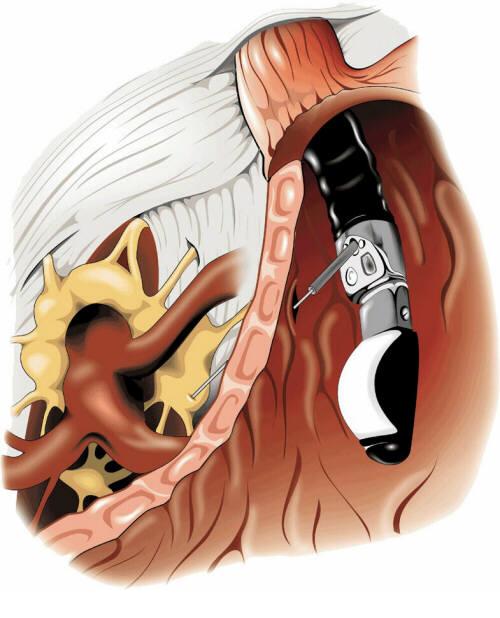
Under direct endoscopic view, the linear EUS instrument is introduced into the stomach to reach the lesser curve in the sub-cardiac area. In this position, the probe is lightly pressed against the gastric wall to obtain a good coupling and a good view of surrounding structures. At this site, it is easy to identify the aorta under the diaphragm which appears as an anechoic tube structure in a longitudinal plane and the origin of the celiac axis is seen beside this. Color Doppler can confirm the vascular landmarks (Figures 3 and 4).
Figure 3. Monochrome visualization of the celiac trunk.
Figure 4. Color Doppler visualization of the celiac trunk.
As previously emphasized, the celiac plexus is not identified as a discrete structure but is located based on its position relative to the celiac trunk.
Two different treatment procedures have been described to perform EUS CPN depending on the device used to perform alcohol injection.
The first technique described uses a standard 22 gauge needle used for all the biopsy procedures under EUS guidance (Figure 5); this is a cutting needle with a removable inner sheet occluding a single hole at the needle tip. For this reason, it is necessary to perform two injections of alcohol at both sides of the trunk in order to obtain an adequate injection of alcohol at both sides of the celiac trunk.
Figure 5. Standard 22 gauge needles.
The second procedure, which is actually more diffused due to its rapidity, uses a new needle (Figure 6) properly designed for this procedure (EUS 20 CPN, Wilson Cook, Winston-Salem, NC, USA); it is a 20 gauge needle with a penetrating tip closed and with some lateral holes which allow a radial diffusion of alcohol to both sides of the origin of the celiac axis with a single injection.
Figure 6. EUS 20 CPN (Wilson Cook, Winston-Salem, NC, USA) needle.
Once the origin of the celiac trunk is located from the sub-cardiac position, the needle (whichever used) is passed through and fixed to the celiac trunk by a luer-lock. Then, under real time control, the needle is released and pushed out from the working channel to trans-pass the gastric posterior wall and is immediately inserted adjacent to the celiac trunk.
At this phase, the two procedures differ slightly, considering the needle position with respect to the celiac trunk; in the first procedure, due to the fact that the needle has only one hole and cannot spray alcohol, the needle tip is positioned by one side of the trunk originating from the aorta and, after having completed the injection, it must be pulled back slightly and again inserted on the other side of the trunk to carry out another injection.
In the second technique, the spraying possibility given by the EUS 20 CPN needle allows the endosonographer to put the needle tip anterior to the basis of the origin of the celiac axis and to carry out only one injection (Figure 7).
Figure 7. EUS image of the needle at base of the celiac trunk.
The injection time is identical for both devices used. When the needle tip is in place, the inner sheet is removed and an aspiration test is performed to rule out vessel penetration before injection.
Then, 3-6 mL of a local analgesic, usually bupivacaine 0.25-0.75%, is injected first followed by 15-20 mL of a neurolytic agent (98%) dehydrate alcohol (Figure 8).
Figure 8. EUS image of lidocaine injection.
The alcohol injection produces an echogenic cloud obscuring the aorta and celiac axis (Figure 9).
Figure 9. EUS image of alcohol injection showing an echogenic cloud obscuring aorta and celiac axis.
In chronic pancreatitis patients, some Authors prefer to use steroids (10 mL or 80 mg (6 mL) triamcinolone) instead of alcohol.
However, in chronic pancreatitis, most results are obtained with alcohol and when traditional techniques were used.
The EUS CPN procedure usually lasts approximately 15 minutes and, during the procedure, arterial pressure has to be monitored because the alcohol injection may produce hypotension and it is necessary to infuse saline solution.
Results
Currently, there are few data about CPN under EUS guidance. However, the results are comparable to other conventional methods used to relieve pancreatic pain with neurolytic agent injections.
The safety and efficacy of EUS CPN has previously been demonstrated as relieving pancreatic pain in a cohort of 25 patients with pancreatic cancer followed for 12 weeks and 5 patients with other intra-abdominal malignant neoplasms [5]. These studies showed a significant decrease of pain at 2, 4, 8 and 12 weeks after EUS CPN.
About 80% of the patients also benefited in a long-term observation (a mean follow up-of 10 weeks) [5]. Other Authors described 58 patients treated in order to palliate pain due to non-operable pancreatic cancer. A short-term decrease of pain was seen in 78% of the patients but the control of pain decreased in 30% at 12 weeks.
Of particular interest is the evidence, reported by Gunaratnam et al. in the widest population reported to have been treated using this modality, that, if the treatment is associated with chemoradiation or chemotherapy, the decrease in the pain score was significantly higher as compared to patients who did not undergo any additional therapy [6] (Figure 10).
Figure 10. Decrease of the pain score according to different treatments. (N Gunaratnam et al. [6], modified).
Up to now, the real role of EUS CPN in the treatment of pain related to chronic pancreatitis is not so clear, lacking enough comparative data comparing EUS CPN and other modalities of treating such multifactorial pain.
Only two studies [7, 8] have tested EUS CPN in this setting; in 90 patients steroids were injected during EUS CPN and a beneficial effect was observed after 7 days in only 55% [7]. Furthermore, in the follow-up of these patients, only 25% still showed a significant decrease in the pain score after 12 weeks [7].
Many authors believe that the difference in results between patients with pancreatic cancer or chronic pancreatitis probably depends on the origin of the pain which can be considered only due to the nervous growing of the tumor in pancreatic cancer and which is multifactorial, with a great psychological impact, in chronic pancreatitis.
Another study described 22 cases of CPN (10 EUS CPN and 12 CT CPN) which showed the benefit in 40% at 8 weeks under EUS guidance (30% at 24 weeks) and in 25% under CT guidance. But the Authors concluded that the number of patients was too limited [8].
There are only a few complications related to the procedure and they are described as only transitory [3]. Orthostatic hypotension or a transient diarrhea may frequently be described.
The infusion of liquid can contrast the hypotension, while the diarrhea is generally auto-limiting and does not exceed 24 hours. Only a few cases of chronic diarrhea have been described; other complications are: peri-pancreatic abscess, reversible paraparesis and a pseudo alcohol-induced aneurysm [9, 10, 11]. To prevent the abscess, it is important to carry out antibiotic prophylaxis.
Conclusions
Celiac plexus neurolysis during EUS appears to be a safe technique, without complications. It seems to control neoplastic pancreatic pain in a short time in about 90% of cases and in a long time in about 30%.
In the management of chronic pancreatitis pain, the role of EUS CPN is not so clear and only 50% of patients have a good reduction of pain within a short period of time. However, only 10% seem to show a benefit at 24 weeks. EUS CPN results seem to be comparable to the results obtained with the other procedures, although the numbers are still too low. An important advantage is that EUS CPN may be performed during bioptic staging of pancreatic cancer [12].
It is also not very clear if there is the possibility of performing more than one procedure of neurolysis.
In summary, EUS CPN is safe and effective for the palliation of patients with pain caused by unresectable pancreatic cancer. Chemotherapy with and without radiotherapy also significantly decreased pain scores.
In addition, the proximity of the posterior lesser curve of the stomach to the celiac plexus, the use of continuous real time visualization of the target area and the availability of the Doppler to assess the vasculature all facilitate accurate needle placement.
CPN under EUS guidance requires further investigation in order to identify the advantages of this approach over conventional percutaneous techniques. The ability to perform the procedure in conjunction with tumor staging and FNA may streamline the care of these patients. The use of EUS CPN earlier in the course of pancreatic cancer to alleviate pain should be encouraged.
References
Levy MJ, Wiersema MJ. EUS-guided celiac plexus neurolysis and celiac plexus block. Gastrointest Endosc 2003; 57:923-9. [More details]
Kappis M. Sensibilitat und lokale Anasthesie im chirurgischen Gebiet der Bauchhohle mit besonderer Berucksichtigung der splanchnicus-Aasthesie. Beitrage zur klinischen Chirurgie 1919; 115:161-75. [More details]
Lee JM. CT-guided celiac plexus block for intractable abdominal pain. J Korean Med Sci 2000; 15:173-8. [More details]
Eisenberg E, Carr DB, Chalmers CT. Neurolytic celiac plexus block for treatment of cancer pain: a meta-analysis. Anesth Analg 1995; 80:290-5. [More details]
Wiersema MJ, Wiersema LM. Endosonography-guided celiac plexus neurolysis. Gastrointest Endosc1996; 44:656-62. [More details]
Gunaratnam NT, Sarma AV, Norton ID, Wiersema MJ. A prospective study of EUS-guided celiac plexus neurolysis for pancreatic cancer pain. Gastrointest Endosc 2001; 54:316-24. [More details]
Gress F, Schmitt C, Sherman S, Ciaccia D, Ikenberry S, Lehman G. Endoscopic ultrasound-guided celiac plexus block for managing abdominal pain associated with chronic pancreatitis: a prospective single center experience. Am J Gastroenterol 2001; 96:409-16. [More details]
Gress F, Schmitt C, Sherman S, Ikenberry S, Lehman G. A prospective randomized comparison of endoscopic ultrasound- and computed tomography-guided celiac plexus block for managing chronic pancreatitis pain. Am J Gastroentero. 1999; 94:900-5. [More details]
Chan VW. Chronic diarrhea: an uncommon side effect of celiac plexus block. Anesth Analg 1996; 82:205-7. [More details]
Navarro-Martinez J, Montes A, Comps O, Sitges-Serra A. Retroperitoneal abscess after neurolytic celiac plexus block from the anterior approach. Reg Anesth Pain Med 2003; 28:528-30. [More details]
Kumar A, Tripathi SS, Dhar D, Bhattacharya A. A case of reversible paraparesis following celiac plexus block. Reg Anesth Pain Med 2001; 26:75-8. [More details]
Varadarajulu S, Wallace MB. Applications of endoscopic ultrasonography in pancreatic cancer. Cancer Control 2004; 11:15-22. [More details]
Article in PDF format
--------------------------------------------------------------------------------
Keywords Celiac Plexus /innervation; Endosonography; Pain; Pancreatic Neoplasms
Abbreviations CPN: celiac plexus neurolysis
CorrespondencePaolo Giorgio ArcidiaconoDivision of Gastroenterology and Gastrointestinal EndoscopyUniversity Vita-Salute San RaffaeleIRCCS San Raffaele HospitalVia Olgettina, 6020132 MilanoItalyPhone: +39-02.2643.2145Fax: +39-02.215.2559E-mail address: arcidiacono.paologiorgio@hsr.it
JOP Home page
- http://www.joplink.net/prev/200407/26.html
Blood Work Questions
Posted by cj on
In Reply to: blood work question?? posted by jeff
Lab Studies:
Blood tests
**Elevations of serum amylase and lipase are found only during acute attacks of pancreatitis, usually early in the course of the disease**In the later stages of chronic pancreatitis, atrophy of the pancreatic parenchyma can result in serum
enzyme levels within the reference range, even during acute attacks of pain.
While low concentrations of serum trypsin are relatively specific for advanced chronic pancreatitis, they are not sensitive enough to be helpful in most patients with mild-to-moderate disease.
Laboratory studies to identify causative factors include serum calcium and triglyceride levels.
When common etiologies are not found, research protocols are available to test for genetic mutations in cationic trypsinogen and CFTR.
Fecal tests
Because maldigestion and malabsorption do not occur until more than 90% of the pancreas has been destroyed, steatorrhea is a manifestation of advanced chronic pancreatitis, and neither qualitative nor quantitative fecal fat analysis can detect early disease.
Assays of fecal chymotrypsin and human pancreatic elastase 1 have the same limitations but are useful in confirming advanced chronic pancreatitis with exocrine insufficiency.
Pancreatic function tests
Direct tests: These tests are the most sensitive and can be used to detect chronic pancreatitis at its earliest stage; however, they are somewhat invasive, labor intensive, and expensive.
Determination in duodenal aspirates: Intubation of the duodenum usually is performed with a Dreiling tube, which allows for separate aspiration of gastric and duodenal contents. The methodology varies depending on the specific laboratory; however, the authors generally use exogenous secretin with cerulein or cholecystokinin to achieve maximal stimulation of the pancreas. The output of pancreatic bicarbonate, protease, amylase, and lipase then is measured in the duodenal aspirates. This test currently only is available in specialized centers. While the greatest sensitivity can be obtained in prolonged infusions of secretagogue to uncover a decreased pancreatic secretory reserve, it is impractical for general clinical use.
Determination in pancreatic juice: This test generally is performed in conjunction with an endoscopic retrograde cholangiopancreatography (ERCP). The pancreatic duct is freely cannulated, an exogenous secretagogue is administered as above, and the pancreatic juice then is aspirated out of the duct as it is produced. The output of pancreatic bicarbonate, protease, amylase, and lipase are measured. This test is gaining popularity because most patients undergo ERCP at some point in their evaluation.
Indirect tests: Noninvasive tests of pancreatic function have been developed for detecting chronic pancreatitis. In principle, these tests work via oral administration of a complex substance that is hydrolyzed by a specific pancreatic enzyme to release a marker substance. The intestine absorbs the marker, which then is measured in the serum or urine. These tests are capable of detecting moderate-to-severe chronic pancreatitis. The presence of renal, intestinal, and liver disease may interfere with the accuracy of these tests. Neither currently is freely available in the
http://www.emedicine.com/med/topic1721.htm
Monday, June 12, 2006
Gary Fry


Gary and Rhonda Fry
Gary Fry August 12 1957 to April 30 2006
On April 30th 2006 Gary Fry passed away leaving behind his much loved wife Rhonda who’s battles with Chronic Pancreatitis was the inspiration for the creation of the Pancreatitis Message Board(PMB). Gary didn’t just create a great place where you posted a message, he created a family atmosphere and welcomed unreservedly anyone who wanted to post and make themselves known. The sense of family and community has always been a special feature of this board and through this Gary helped so many people who suffer pancreas related problems many of whom may never have actually made a post on the board but read often. He also kept it going through some very hard times but he had enough compassion/kindness in him to realize how much the many members of the community he had created depended on his board and he chose never to give up on it. Gary you are much loved and will be sorely missed,
I struggled to write about what Gary meant to the many people who frequent the PMB. So the best way I could think of was to take a selection of the many posts and e-mails that accompanied the sad news of Gary’s death.
From Alma
I first met Gary in the mid to late 90’s. I had been diagnosed with chronic pancreatitis in 1995 and was playing around on the computer learning how to navigate the internet. I found a site made by a person by the name of Bruce. His site was nothing but pancreas information and stories. I cried like a baby when I read the stories of others who had chronic pancreatitis. It was like finally someone could to relate and understand what I was going through. There was a link to other sites on Bruce’s site and I went through all of them. On one of the links I clicked on I immediately knew I had found a safe haven. I emailed Gary and we emailed each other back and forth and he had a message board he had started so his wife Rhonda could have someone to talk with that knew what she was going through. It was like we clicked immediately as friends. On the first message board there was not a lot of us and what there was instantly felt like family members that had known each other all their lives.
Gary showed me how to make a web site using a site on the internet that helps you do it. I still had questions and he would help me with them. I learned a lot from Gary not only about message boards and web pages but about life in general. His wife was very ill quite often but he never once complained to me about it. He always wanted to be there for her and was always there for her.
Another thing that brought Gary and myself together is a common love for Bluegrass Music. We both loved the bluegrass sound so we not only had pancreatitis in common but we were both country hicks and we loved this style of music. I even sent him a tape one time of a song I sang to get him to let me know how I was doing. He was honest and helpful. I never will be a true singer but he saw and understood that singing Southern Gospel which includes some bluegrass music, was for me a way to worship my God. Not many people understand that but Gary did from the beginning.
We contacted each other every day for some reason or another, be it me learning how to make web pages or dealing with the pain of cp or just a friendly chat to pass the time. We quickly became like brother and sister. We had our ups and downs like siblings also but we never ever gave up on each other. I will miss him terribly as I know his family will too. Family came first with him and he loved Rhonda with all his heart and more if it was possible. He was ever mindful that Mike could be sent to Iraq and worried about that a lot in the past couple of yrs.
Gary was always supportive of those that posted on the message boards he made. He did not put up with arguing and many times I myself would get in trouble for posting in an argumentative way. Being a very close friend did not stop him from scolding me either. Most times he scolded me in a private email and I really appreciated him for that. He was our rock of Gibraltar when we needed him to be and I don’t see how the board will function without him. I know it will never be the same with him gone. I never dreamed in a million years he would pass on before I did because I was the one with pancreas problems not him. It was a huge shock to find out he had died. Although I had not heard much from him lately I will miss him terribly. Just knowing he was there should I want to email him gave me a sense of security. That security is gone now and there will never be another Gary Fry for me nor will any of the message boards I see on the internet compare in any way to Gary’s board. In honor of him we are keeping the board he made up and running. It is different from other message boards on the internet in the fact that it is not censored. You can say what you want within reason and we all feel like one big family. The board has gotten larger each year and that is because Gary allowed it to be a family oriented board without having to have passwords and approval of a post, etc. I will always hold near to my heart the memories of Gary and his love for Rhonda and Bluegrass Music.
"THANK YOU GARY FOR YOUR CREATION OF THIS BOARD AND LOVE AND SUPPORT YOU HAVE GIVEN ALL OF US."
“It hasn't been easy I know, but you kept right on doing what you could to inform anyone who needed information about chronic pancreatitis. You will never be forgotten.”
Alma
aka: firstwin
Posted by Cindy on May 08, 2006
Taken from an e-mail from Gary to Cindy this was sent to me as is shown here:
“This group is the first to have a Pancreatitis specific message board on the internet. It is the longest running Pancreatitis specific message board as well. I started it in June of 1997 on a different server than it is now. We have moved several times due to different circumstances., usually the server shutting down.”
From Gary’s Sister DiAnn
“I have something that you may like to read about him. It will definitely give you and idea what kind of person he was . He worked in the coal mines and when there was an explosion he was there more than once to help and at times it got pretty gruesome.”
“In 1997 while he was going to college he was one of two people to receive a scholarship called the Felton Patton Memorial Scholarship”
The people on the Pancreatitis were an extended family to him and when we talked he often talked about the people on the board as if I should know them. I did get to the point that I felt like I knew some of them….”.
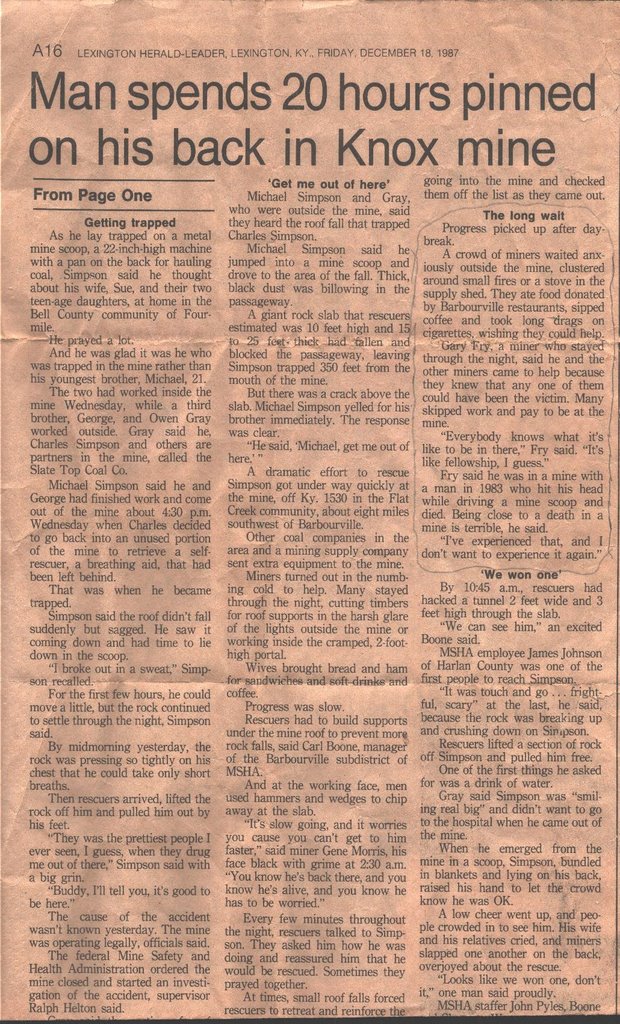
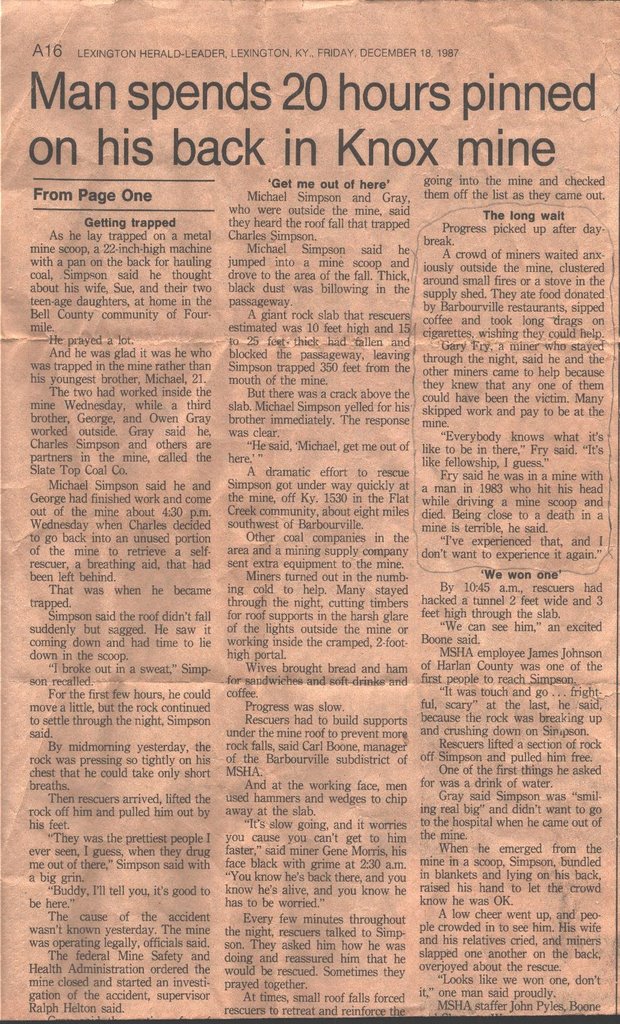{kind=link}
The excerpt on the right is from the paper clipping below
Subject: Re:Official Resignation as Administrtaor - CJ (c.j.) is new Administrater.
From: Gary
To: All
Date Posted: 21:12:15 12/14/05
Message:
“Wow ALma; I don't know where to start! It has been a two way street, we have been there for each other I think. We probably have been more like family, because we, as many do not know, have had our own ups and downs, (very few and nothing really serious), behind the scene and off the board. But like family, we have always healed our wounds and been able to forgive each other and go forward and leave the past behind. But most of all we were there for each other through the very tough times and we laughed a lot at the good times. I think we have even laughed at our self sometimes :)……”
Posted by Larry on May 02, 2006
I just received an email from Mike Fry who stated his father, Gary Fry, passed away this passed Sunday. If this is true, it is truly a very sad moment for all of us.
Can someone else verify this for us? There was an email address in the email that I received that I may respond back to.
I apologize if this seems so blunt, but I really did not know Gary was doing so bad.
Posted by Chuck on May 02, 2006
I just called the information line at Hampton Funeral Home in Barbourville. Gary Lee Fry did indeed die on Sunday. His funeral will be held Thursday at 1 PM.
I am so sorry to confirm the notice from his son. Gary was a very special person. He put his heart and soul into starting and running this board when Rhonda first was diagnosed. He has been a good friend and will be sorely missed.
Rest in Peace, Buddy.
Chuck
Posted by Brett on May 03, 2006
“Rhonda if you are reading this then please accept my condolences. Gary was a special person who has had a huge impact in my life by providing this special place. For that I am eternally grateful and forever in his debt. I can only imagine the pain you are in and hope that you will find peace for yourself.”
Rest in peace Gary, you will be missed
Posted by Pete on May 03, 2006
“I am truly saddened by Gary's untimely passing. He corresponded with me quite often when I joined this board in July'04.I will be forever grateful for him starting this board.Rhonda...if you read this, please accept my heartfelt sympathies for your loss. You will be in my prayers. I know Gary will be watching over us now from above. God has a special plan for him. I am truly going to miss him...a fine measure of a man!”
Pete(Fla.)
Posted by Christine on May 03, 2006
“i just want to offer my deepest condolences to Gary’s wife and family. i am so grateful to him for all his hard work with this board. it has been a life saver and he has made a difference in so many peoples lives that are suffering with this. i am so, so sorry. thank you Gary, rest in peace.“
Posted by Trisha on May 03, 2006
“What can i say that's not already been said. My thoughts and prayers go out to all his family and friends.I don't honestly know were i would be today if i never found this message board. Gary has helped everyone of us and that say's something about a person.
Rest in peace Gary......Thanks.”
Posted by Pam on May 03, 2006
“My sympathies as well. I saw that Gary last posted on 4/18...he seemed uplifted that this board was active. I hope that gave him joy and peace.”
Pam
Posted by Diane on May 03, 2006:
"REST IN PEACE... a special thank you for this board Gary... from those that post and those that come here as I do to, just read and learn. You and this board have given so much to those who suffer from this horrid disease. Deepest regrets to Rhonda and all that love you."
Diane
Posted by Christine Stanborough on May 03, 2006:
“RhondaTo say Gary was special is such an understatement. God bless you Rhonda your loss is immense and I just hope that our words give you some comfort. You and your family are in our thoughts and prayers.”
Kind regardsChristine
Posted by laurie on May 03, 2006:
“I just want to add my condolences to his family and friends. I am also shocked and profoundly saddened. I missed his posts but took it for granted that he was always going to be here to keep in touch with his legacy.
As far as the board goes with Carol....I think because it was his decision to dedicate this board to her memory that it should be respected. I think that it is a tribute to the person he was that he did this and to change it now would somehow not honour his wishes. Unless of course, there are other issues that his family wish to address. Just my thoughts, such as they are....”
laurie
Posted by Vickie on May 03, 2006:
.”Gary, we've had many conversations down the years and you've been a wonderful friend”
Vickie
Posted by judylu on May 03, 2006:
“I only hope he is at peace now. My heart goes out to Rhonda and the rest of his family and friends. He is surely missed and will be remembered well.”
Posted by Tami on May 04, 2006:
“I found this board in September of last year, and it has been my salvation with this disease. To find so many other people that can truly relate and sympathize as to what you are going through is not only priceless, but very much needed. Gary is and always will be a true hero to me, to stand so vigilantly by his wife’s side during her illness, to offer so much support and knowledge to others going through CP, what a true saint. Rhonda, I don't know you personally, but I am very sorry for what you are going through, your husband loved you so very much and you could just hear it in every word he had to say about you. You and your family are in my prayers, and I will pray for strength during this very difficult time.”
Tami McClurg
Posted by Lorie on May 03, 2006:
“I did not want to come on the board this morning, I waited 2 hours for fear of knowing that Gary has passed away. My heart hurts and goes out to Rhonda and all of Gary's family. Rhonda if you are reading the board please know that my heart goes out to you. I would like for you to know how much Gary has meant to me. Gary was my salvation in 1997 when I found the Pancreatitis message board. I felt alone and confused over my disease. I had so many questions, fears and needed desperately to know what all of this meant and if anyone else was feeling what I was feeling. My husband is supportive, but I don't know that anyone can imagine how we all feel unless you actually walk in our shoes.Gary brought all of us together as a family, none of us would even know each other if Gary had not brought us together with this board. For this we will always remember Gary and for me he will always hold a very special place in my heart. I can't even begin to say everything I am thinking right now. I am still so very shocked. Rhonda you more then anyone knows how much Gary loves you, he is one the most supportive husbands I know he always talked about you with so much love in his heart.Gary, and his passion for music brought joy to many lives. Gary, will be missed greatly. He had a way of sharing his passion's in life through the web. I know God has a plan for him and he is looking over all of us
Rest in peace Gary, Rest in peace.
My condolences to all of Gary's Family.”
Lorie Bledsoe
From CJ
I came across "
From Cindy
“Cant even express to Gary/Rhonda how much the creation of the board has meant to me. Like the rest of you know having this condition that those that don’t have it just can’t understand you 100% and what going thru. This place to come-the board has become over the years with some like extended family to me and to my son Brandon even if we live states/country away like we are so close. I have gained some good friends thru this board including Gary and if it wasn’t for him that would never be-we would have never been brought together for a life of friendship. And one day when Brandon is older and knows/understands my condition and friends over the years he will know about 'Uncle Gary' as well.
Gary you will be missed”
Cindy M
Posted by Cindy on May 08, 2006:
“I came on the board/around since 99. As a lot of you know being the first later on to get pregnant with CP and a lot of you went thru each step with me especially the ups and downs and when I was in the hospital 1 1/2 months while pregnant. For me I would like something said for Gary having to do with that and what he wrote to me when he resigned from board to only be a user of it because some of you called yourselves/I called you 'aunt/nana' and him Uncle Gary he said to Brandon which shows the closeness, caring etc. He called me in the hospital too and helped me with some ?s and worries I had, always included him on emails w/pictures of brandon growing up now 2 1/2 + and he always wrote back such nice things but this one I found hits home and even the part for us to be there/help CJ he knew and went thru some rough times with the board and stuck it out/did what he had to do and best for the board up till when he felt he had to resign. Gary/Uncle Gary -you will be missed tremendously”
Cindy and Brandon
Posted by Gary on December 17, 2005 at 13:02:49:
Cindy;“You, I will never forget. You will always be our first member to deliver a baby, little Brandon, in our group of Pancreatitis sufferer's here. You have always and will always be a friend. Say hello to Brian and little Brandon. Keep in touch. And most of all, lets all help C.J., it is a pretty rough job at times”.
Gary
Finally this was posted by Joan and I thought it was a great way to finish
Posted by Joan on May 12, 2006
I ran across this poem today and when I read it made me think of Gary so I thought I would share it with you guys....
THE BROKEN CHAIN
We little knew that morning that God was going to call your name.
In life we loved you dearly; in death we do the same.
It broke our hearts to lose you, you did not go alone;
for part of us went with you, the day God called you home.
You left us peaceful memories, your love is still our guide;
and though we cannot see you, you are always at our side.
Our family chain is broken, and nothing seems the same;
but as God calls us one by one, the chain will link again.
Author Unknown
Sunday, June 11, 2006
Medical Malpractice
Each year, over 100,000 people are killed by preventable medical errors, due to negligence or wrongdoing. Many more are seriously or permanently injured, disfigured or disabled.The leadership in the House of Representatives is promoting legislation, written by the insurance industry and HMOs, which would restrict the ability of Americans injured by medical malpractice to hold accountable those who caused them harm.
The legislation would create a "one size fits all" system for people injured in a medical setting or nursing home. The limits would apply no matter how severe the harm - even if the wrong limb was amputated, an unnecessary mastectomy was performed, or even in cases involving the death of a child. Congress has their priorities mixed up. Shouldn't we be talking about protecting the health and safety of patients, rather than protecting Congress' corporate friends in the health care, insurance and HMO industries.Urge Congress to oppose any legislation seeking to restrict the rights of people through so-called medical malpractice "reform."
http://www.thepetitionsite.com/takeaction
/991264371?z00m=88688&z00m=88688<l=1149961706
The legislation would create a "one size fits all" system for people injured in a medical setting or nursing home. The limits would apply no matter how severe the harm - even if the wrong limb was amputated, an unnecessary mastectomy was performed, or even in cases involving the death of a child. Congress has their priorities mixed up. Shouldn't we be talking about protecting the health and safety of patients, rather than protecting Congress' corporate friends in the health care, insurance and HMO industries.Urge Congress to oppose any legislation seeking to restrict the rights of people through so-called medical malpractice "reform."
http://www.thepetitionsite.com/takeaction
/991264371?z00m=88688&z00m=88688<l=1149961706
Wednesday, May 31, 2006
The truth about Headaches
Dr. David Buchholz: The Truth about Headaches
By The 700 Club
CBN.com – If you're like most people, you're probably confused about the whole subject of headaches. You may wonder, Do I have migraine? Or do I have a brain tumor? Could it be an aneurysm? What about my tension headaches? Or sinus headaches? Is it arthritis in my neck, or a pinched nerve, or am I just stressed out, or is it my hormones, or what is it? You're not the only one confused and frustrated about headaches.
All headaches arise from a single mechanism - the mechanism of migraine - which generates painful blood vessel swelling when activated by specific triggers. This headache-generating mechanism, which produces not only headaches but also other symptoms including dizziness, neck stiffness, sinus congestion and many more, can be controlled. Control starts with reducing your exposure to some of the triggers, especially certain food and medications. If trigger avoidance alone isn't effective, preventive medication, which blocks the mechanism, can be added. Painkillers, on the other hand, lead you to lose control. Many headache sufferers spin farther and farther out of control in a vicious cycle of victimization by headaches and dependence on painkillers.
DIETARY TRIGGERSDr. Buchholz says there are many unavoidable or difficult to avoid migraine triggers such as barometric pressure and weather changes, hormonal fluctuations, sensory stimuli, physical exertion, sleep deprivation, and stress. With these triggers there is little you can do to avoid these situations. There are however avoidable triggers in which you can begin to take control of your headaches. Avoidable triggers are for the most part, things that are swallowed: certain foods and beverages, and medications. Some potential dietary triggers are listed below. Dr. Buchholz cautions that everyone is different, and it may be that not every one of the foods and beverages that most commonly cause headaches is a trigger for you.
Avoidable dietary triggers.
- Caffeine - Coffee, tea, iced tea and cola. Even decaf coffee and tea may be a problem. Try caffeine-free tea without citrus and other trigger flavors.
- Chocolate - White chocolate (no cocoa) is okay; carob is questionable.
- Processed meats and fish - Aged, canned, cured, fermented, marinated, smoked, tenderized - or preserved with nitrites or nitrates.
- Cheese and other dairy products - The more aged, the worse. Permissible cheeses include cottage cheese, ricotta, cream cheese and good-quality American cheese.
- Nuts - Avoid all kinds, as well as nut butters. Seeds are okay.
- Vinegar - Clear or distilled vinegar is allowable. Don't overdo condiments made with vinegar such as mustard.
- Certain fruits and juices - Citrus fruits and their juices as well as bananas and dried fruit preserved with sulfites.
- Certain vegetables - Avoid onions, sauerkraut, pea pods and certain beans.
- Aspartame - Nutrasweet and saccharin. Sucralose (Splenda) isn't a problem.
- Fresh yeast-risen baked goods - Less than one day old: homemade or restaurant baked breads such as sourdough.
PREVENTION OF HEADACHESBeyond dietary modification, you can make other lifestyle choices to help control your headaches. Regularity is key: you should sleep, eat and exercise on a regular basis. Get enough sleep each night, seven to eight hours or more, and don't oversleep sporadically, as on weekends.Skipping meals is a common trigger for migraine. Stay on schedule for three meals a day, no more than six to eight hours apart. Snack in between if you wish, but only on nonrestricted items. Exercise helps both body and mind, and in both ways helps to control headaches. Regular exercise is a means of relieving stress and thereby helps in reducing your trigger load. Exercise also enhances your migraine threshold by stimulating endorphins in your brain and helping to block the mechanism that causes headaches.
Friday, May 26, 2006
Enzymes
Posted by Cindy on May 26, 2006
Digestion begins in the mouth where we physically break down foods with our tongue and teeth. The food particles then travel to the stomach where they are further digested by the acidic stomach juices.As food leaves the stomach and enters the small intestine, several digestive fluids are added. These fluids contain enzymes, which aid in the digestive process.For example, the pancreas secretes three enzymes into the small intestine: amylase, protease, and lipase. These enzymes are also produced by the intestinal wall. We also get important enzymes from the foods we eat. However modern cooking practices and food processing kills many of these enzymes before we ingest them. This lowers the amount of enzymes in our digestive system and slows the digestive process.Many people take supplements that contain plant enzymes that catalyze, or stimulate, the digestion process. These supplements often contain amylase, protease and lipase - enzymes that help take some of the work away from organs like the pancreas, which may be under undue stress due to modern eating habits.Each of these enzymes have special binding spots called receptors that help it match with and bind to a particular type of nutrient.For example amylase digests carbohydrates such as the starches found in potatoes and pasta. Proteases help the body break down protein found in foods such as meat into tiny building blocks that can then be used to build and maintain the body's tissues. And lipases help the body break down fats and oils, which may help lower the amount of fats circulating in your blood stream.http://digestive.healthcentersonline.com/liverpancreasbiliary/then under Animations click on Enzymes.
Digestion begins in the mouth where we physically break down foods with our tongue and teeth. The food particles then travel to the stomach where they are further digested by the acidic stomach juices.As food leaves the stomach and enters the small intestine, several digestive fluids are added. These fluids contain enzymes, which aid in the digestive process.For example, the pancreas secretes three enzymes into the small intestine: amylase, protease, and lipase. These enzymes are also produced by the intestinal wall. We also get important enzymes from the foods we eat. However modern cooking practices and food processing kills many of these enzymes before we ingest them. This lowers the amount of enzymes in our digestive system and slows the digestive process.Many people take supplements that contain plant enzymes that catalyze, or stimulate, the digestion process. These supplements often contain amylase, protease and lipase - enzymes that help take some of the work away from organs like the pancreas, which may be under undue stress due to modern eating habits.Each of these enzymes have special binding spots called receptors that help it match with and bind to a particular type of nutrient.For example amylase digests carbohydrates such as the starches found in potatoes and pasta. Proteases help the body break down protein found in foods such as meat into tiny building blocks that can then be used to build and maintain the body's tissues. And lipases help the body break down fats and oils, which may help lower the amount of fats circulating in your blood stream.http://digestive.healthcentersonline.com/liverpancreasbiliary/then under Animations click on Enzymes.
Thursday, May 11, 2006
Dangers of Too Much Acetaminophen!
Dangers of Too Much Acetaminophen!
Acetaminophen (APAP) is the most widely used analgesic (pain killer). It is available in various formulations including: liquid, tablet, capsule, and suppository. APAP has an excellent safety profile when ingested appropriately, but liver toxicity can develop in acute overdoses or chronic ingestions.
Over-the-counter combination products can be have hidden dangers especially if multiple medications containing acetaminophen are taken together. Unfortunately, initial signs and symptoms of acetaminophen toxicity are non-specific (nausea and vomiting) or absent. To avoid liver damage from acetaminophen, do not take more than 1 gram (1,000mg) of acetaminophen at once, do not exceed 4 grams of acetaminophen in 24 hours, and always check to see if over-the-counter or prescription medications contain acetaminophen. For children, do not exceed 10-15mg/kg/dose of acetaminophen and do not exceed five doses or 2.6 grams in 24 hours. If you are unsure about any medication containing acetaminophen, contact the poison center at 1-800-222-1222.
Scenarios which often result in inadvertent acetaminophen overdose include:
Reasons for unintentional overdoses appear to be multi-factorial and include:
Common prescription medications containing Acetaminophen include:
Common over-the-counter preparations containing Acetaminophen:
Acetaminophen
Tylenol, Non Aspirin Pain Relief, Tylenol Children’s, Tylenol Infants, Tylenol Sore Throat
Acetaminophen and Diphenhydramine
Excedrin PM, Tylenol PM, Legatrin PM, Sominex Pain, Tylenol Severe Allergy, Anacin PM Aspirin Free
Acetaminophen and Pseudoephedrine
Alka Seltzer Plus Cold and Sinus, Children’s Tylenol Sinus, Infant’s Tylenol Cold, Sinutab Sinus Maximum Strength Without Drowsiness, Sudafed Cold and Sinus, Sudafed Sinus Headache
Acetaminophen and Aspirin and Caffeine
Excedrin, Genaced, Goody’s Extra Strength Headache Powder, Vanquish Extra Strength Pain Reliever
Acetaminophen and Pseudoephedrine and Chlorpheniramine
Alka Seltzer Plus Cold, Children’s Tylenol Cold, Comtrex Allergy Sinus, Thera-Flu Flu and Cold, Sinutab Sinus Allergy
These are just some of the many preparations containing acetaminophen on the market.
This is taken from Minnesota Poison Control Center web site
Acetaminophen (APAP) is the most widely used analgesic (pain killer). It is available in various formulations including: liquid, tablet, capsule, and suppository. APAP has an excellent safety profile when ingested appropriately, but liver toxicity can develop in acute overdoses or chronic ingestions.
Over-the-counter combination products can be have hidden dangers especially if multiple medications containing acetaminophen are taken together. Unfortunately, initial signs and symptoms of acetaminophen toxicity are non-specific (nausea and vomiting) or absent. To avoid liver damage from acetaminophen, do not take more than 1 gram (1,000mg) of acetaminophen at once, do not exceed 4 grams of acetaminophen in 24 hours, and always check to see if over-the-counter or prescription medications contain acetaminophen. For children, do not exceed 10-15mg/kg/dose of acetaminophen and do not exceed five doses or 2.6 grams in 24 hours. If you are unsure about any medication containing acetaminophen, contact the poison center at 1-800-222-1222.
Scenarios which often result in inadvertent acetaminophen overdose include:
- Children being given Tylenol Children’s to relieve a fever over several days
- Treating pain (headache, toothache, backache etc.) with various prescriptions and over-the-counter pain medications
- Treating a cold, allergies, and stuffed-up nose at the same time
- Ingesting various generic non-aspirin products
Reasons for unintentional overdoses appear to be multi-factorial and include:
- Simultaneous use of multiple products containing APAP
- Inadvertently exceeding the maximum daily dose of 4 grams (4,000mg) of APAP in adults or 2.6 grams (2,600mg) of APAP in children
- Unaware of various over-the-counter (OTC) products that contain APAP
- Co-ingesting OTC’s and prescription medications that contain APAP
Common prescription medications containing Acetaminophen include:
- Acetaminophen and Hydrocodone (Vicodin, Lortab)
- Acetaminophen and Propoxyphene (Darvocet)
- Acetaminophen and Oxycodone (Percocet, Endocet, Roxicet)
- Acetaminophen and Tramadol (Ultracet)
- Acetaminophen and Butalbital and Caffeine (Fioricet)
- Acetaminophen and Isometheptene and Dichloralphenazone (Midrin)
Common over-the-counter preparations containing Acetaminophen:
Acetaminophen
Tylenol, Non Aspirin Pain Relief, Tylenol Children’s, Tylenol Infants, Tylenol Sore Throat
Acetaminophen and Diphenhydramine
Excedrin PM, Tylenol PM, Legatrin PM, Sominex Pain, Tylenol Severe Allergy, Anacin PM Aspirin Free
Acetaminophen and Pseudoephedrine
Alka Seltzer Plus Cold and Sinus, Children’s Tylenol Sinus, Infant’s Tylenol Cold, Sinutab Sinus Maximum Strength Without Drowsiness, Sudafed Cold and Sinus, Sudafed Sinus Headache
Acetaminophen and Aspirin and Caffeine
Excedrin, Genaced, Goody’s Extra Strength Headache Powder, Vanquish Extra Strength Pain Reliever
Acetaminophen and Pseudoephedrine and Chlorpheniramine
Alka Seltzer Plus Cold, Children’s Tylenol Cold, Comtrex Allergy Sinus, Thera-Flu Flu and Cold, Sinutab Sinus Allergy
These are just some of the many preparations containing acetaminophen on the market.
This is taken from Minnesota Poison Control Center web site
Wednesday, April 12, 2006
Top Ten Reasons to Fire your Doctor
Posted by cj on April 11, 2006 at 14:58:28:
Top 10 Reasons To Fire Your DoctorGuide Picks
Doctors have strengths and weaknesses. How does your doctor's "bedside manner" match up with your personality?
Are you confident in your doctor's ability? Do you feel that you understand the directives and decisions made by your doctor? Are you encouraged to ask questions? Is the overall experience at your doctor's office positive?
The relationship between a doctor and patient is very important. If you're answering no to most of the questions it may be time for a change.
1) Lack Of Confidence In Doctor's AbilityA patient must trust their doctor. Patients are more likely to be compliant with their treatment plan if they have confidence in their doctor's ability. A patient consults with a doctor for their expertise as a diagnostician and ability to problem-solve. A patient should not routinely leave the doctor's office feeling uneasy about decisions and recommendations which are made by the doctor. If you find yourself doing that, it may be time to fire your doctor.
2) Lack Of Continuity Between VisitsThe nature of chronic illness implies you will be seeing a doctor many times to help you manage your condition. With copious notes in your medical chart, your doctor should be able to recall your prior visit and gauge your progress. Doctors are busy and they see many patients, so it's not always perfect. If you constantly have to repeat yourself and if you feel that your doctor isn't following along, it may be time to fire your doctor.
3) Questions Are Not WelcomePatients go to doctors in search of answers. Patients want answers to:
what's wrong with me? how are we going to treat the condition? what can I expect? what are my options?
Some doctors allow a reasonable amount of time for patient questions. Other doctors are unapproachable and discourage questions. If it's difficult to have a dialogue with your doctor about your health care, it may be time to fire your doctor.
4) Doctor Is Not Forthcoming Does your doctor share all pertinent diagnostic test results with you? Does your doctor share why a specific test is being ordered or why a specific treatment plan has been chosen over another? For example:
Your doctor may give you an order for an MRI. Your doctor may tell you why you need to have an MRI and explain what he is trying to rule out, and then give you the order for the MRI.
If you feel uninformed more often than not, it may be time to fire your doctor.
5) Doctor Is Cold And UnsympatheticIt's important that you understand your doctor, but it is equally important that you be understood by your doctor. Does your doctor understand how your medical condition impacts various aspects of your life? Is your doctor sympathetic about your problem or is your doctor's demeanor cold and abrupt? You must feel that your doctor truly cares about your well-being, otherwise it may be time to fire your doctor.
6) Excessively Long Wait To Get An AppointmentYou may encounter a long waiting period when you try to set up a doctor appointment. Doctors have very busy schedules, especially specialists and surgeons. As the joke goes - I wouldn't want to go to a doctor who will see you the next day. A busy doctor is often a popular doctor with a great reputation. However, by waiting too long for an appointment, you may be compromising your health. If the wait seems unreasonable, find another doctor.
7) Doctor Is Always Rushed Do you have your doctor's full attention during your appointments, or do you sense that your doctor's mind is cluttered by other matters unrelated to you? Do you feel that you're being hurried? Has your doctor ever backed out of the room before you were able to ask all of your questions? If you are left feeling that not enough time is devoted to you during your appointments, it may be time to fire your doctor.
8) Inconvenient LocationIt can be stressful and inconvenient to have to drive a long distance to see your doctor, especially if you have mobility problems. Some patients who live in rural areas have fewer options, but convenience is a factor to be considered. Where will the doctor send you for blood tests, x-rays, and other tests? What are your doctor's hospital affiliations? Be sure your situation is either convenient or agreeable to you, otherwise you may want to find another doctor.
9) Cost / CoverageIf your insurance does not cover your doctor's fees, it is unlikely you would want to stay with that doctor. Know the details of your individual health plan and be certain that your doctor is available to you on the provider list. If not, you may want to find another doctor so your medical costs will be covered by your insurance.
10) Doctor Is Not RespectfulIs your doctor harsh when speaking to you? Does your doctor consider your fears and apprehension when making decisions, or are your feelings disregarded? Does your doctor respect that your time is as important as their own, or does your doctor leave you languishing in the waiting room for unreasonably long periods of time? Do you feel respected as a person by your doctor? If not, it may be time to fire your doctor.
Related ResourcesHow Would You Rate Your Doctor? Should You Change Your Doctor? How To Choose The Right Doctor Last update 4/1/06
Top 10 Reasons To Fire Your DoctorGuide Picks
Doctors have strengths and weaknesses. How does your doctor's "bedside manner" match up with your personality?
Are you confident in your doctor's ability? Do you feel that you understand the directives and decisions made by your doctor? Are you encouraged to ask questions? Is the overall experience at your doctor's office positive?
The relationship between a doctor and patient is very important. If you're answering no to most of the questions it may be time for a change.
1) Lack Of Confidence In Doctor's AbilityA patient must trust their doctor. Patients are more likely to be compliant with their treatment plan if they have confidence in their doctor's ability. A patient consults with a doctor for their expertise as a diagnostician and ability to problem-solve. A patient should not routinely leave the doctor's office feeling uneasy about decisions and recommendations which are made by the doctor. If you find yourself doing that, it may be time to fire your doctor.
2) Lack Of Continuity Between VisitsThe nature of chronic illness implies you will be seeing a doctor many times to help you manage your condition. With copious notes in your medical chart, your doctor should be able to recall your prior visit and gauge your progress. Doctors are busy and they see many patients, so it's not always perfect. If you constantly have to repeat yourself and if you feel that your doctor isn't following along, it may be time to fire your doctor.
3) Questions Are Not WelcomePatients go to doctors in search of answers. Patients want answers to:
what's wrong with me? how are we going to treat the condition? what can I expect? what are my options?
Some doctors allow a reasonable amount of time for patient questions. Other doctors are unapproachable and discourage questions. If it's difficult to have a dialogue with your doctor about your health care, it may be time to fire your doctor.
4) Doctor Is Not Forthcoming Does your doctor share all pertinent diagnostic test results with you? Does your doctor share why a specific test is being ordered or why a specific treatment plan has been chosen over another? For example:
Your doctor may give you an order for an MRI. Your doctor may tell you why you need to have an MRI and explain what he is trying to rule out, and then give you the order for the MRI.
If you feel uninformed more often than not, it may be time to fire your doctor.
5) Doctor Is Cold And UnsympatheticIt's important that you understand your doctor, but it is equally important that you be understood by your doctor. Does your doctor understand how your medical condition impacts various aspects of your life? Is your doctor sympathetic about your problem or is your doctor's demeanor cold and abrupt? You must feel that your doctor truly cares about your well-being, otherwise it may be time to fire your doctor.
6) Excessively Long Wait To Get An AppointmentYou may encounter a long waiting period when you try to set up a doctor appointment. Doctors have very busy schedules, especially specialists and surgeons. As the joke goes - I wouldn't want to go to a doctor who will see you the next day. A busy doctor is often a popular doctor with a great reputation. However, by waiting too long for an appointment, you may be compromising your health. If the wait seems unreasonable, find another doctor.
7) Doctor Is Always Rushed Do you have your doctor's full attention during your appointments, or do you sense that your doctor's mind is cluttered by other matters unrelated to you? Do you feel that you're being hurried? Has your doctor ever backed out of the room before you were able to ask all of your questions? If you are left feeling that not enough time is devoted to you during your appointments, it may be time to fire your doctor.
8) Inconvenient LocationIt can be stressful and inconvenient to have to drive a long distance to see your doctor, especially if you have mobility problems. Some patients who live in rural areas have fewer options, but convenience is a factor to be considered. Where will the doctor send you for blood tests, x-rays, and other tests? What are your doctor's hospital affiliations? Be sure your situation is either convenient or agreeable to you, otherwise you may want to find another doctor.
9) Cost / CoverageIf your insurance does not cover your doctor's fees, it is unlikely you would want to stay with that doctor. Know the details of your individual health plan and be certain that your doctor is available to you on the provider list. If not, you may want to find another doctor so your medical costs will be covered by your insurance.
10) Doctor Is Not RespectfulIs your doctor harsh when speaking to you? Does your doctor consider your fears and apprehension when making decisions, or are your feelings disregarded? Does your doctor respect that your time is as important as their own, or does your doctor leave you languishing in the waiting room for unreasonably long periods of time? Do you feel respected as a person by your doctor? If not, it may be time to fire your doctor.
Related ResourcesHow Would You Rate Your Doctor? Should You Change Your Doctor? How To Choose The Right Doctor Last update 4/1/06
Sunday, April 02, 2006
PAIN MYTHS
Myth #1: "It's only subjective." Pain is a subjective construct and each individual learns the meaning of pain through early life experiences (Merskey & Bogduk, 1994). In science, an objective phenomenon is one that is "perceptible to the external senses," (Dorland's, 1994, p. 1166) while a subjective phenomenon is one that pertains to or is "perceived only by the affected individual; not perceptible to the senses of another person" (Dorland's, 1994, p. 1595). Behavioral observations and patient self-report indirectly measure subjective phenomena; direct methods, e.g., laboratory tests or radiology films, can measure objective phenomena. Physicians treat about 70% of all patients for subjective complaints (Harsha, 1990), so chronic pain patients are hardly unusual. What makes chronic pain patients unique is that they generally do not get better spontaneously. Indeed, they often do not get better after considerable intervention, especially after incorrect treatment strategies...................
For the full article follow this site......Countering Chronic Pain Myths
Friday, March 17, 2006
Enzymes
Plant Enzymes & Probiotics Active Ingredients(Each 1/4 tsp. or gram)
Alpha & Beta Amylase –3,150 DUProteases – 20,500 HUTLipase – 265 LUCellulase – 110 CUHemicellulase – 100 HCUBromelain – 20,000 FCCProbiotic (Bacillus coagulans) – 600 Million CFU
Nutritional InformationCrude Protein- 5.0% min.,Crude Fat- 0%,Crude Fiber- 0%,Moisture- 6.0% max.
Contains no lactose, sugars or preservatives. Add 1/4 teaspoon to each cup of food Plant enzymes: $10.75
Digestive enzymes are special types of protein molecules that catalyzethe breakdown of food into components that can be utilized by the body.These proteins are not stored in the body but are released based on theanticipation aroma or actual presence of food in the digestive system.Because they are not stored they must be taken with each meal,preferably with the food. Merritt's enzymes contain a blend of plant andmicrobial produced enzymes. None of them are from animal sources.
Each enzyme is highly specific as to the class of food it works on andthe temperature and pH of its effective range of activity. Animalderived enzymes will work in only one area of the digestive system,while plant and microbial enzymes work throughout the whole system, frommouth through the stomach into the intestines. As the body ages lessenzymes are produced and supplementation is necessary to assure optimumhealth.
To maintain optimum health in an animal it needs to be fed an optimum,diet, but also needs to have digestive efficiency necessary toassimilate the food ingredients. The digestive efficiency can be reducedby stress of any sort, excitement , anxiety (travel separation, workingstress and so on. To insure optimum digestion and health we recommendthe addition of this supplement to each meal. For optimum utilizationthe supplement should be added to the food and should be moistenedshortly before feeding to be effective.
Since Merritt's enzymes are derived from plant and microbial sourcesthey are active throughout the whole gastrointestinal tract not in aspecific section, as animal derived enzymes are. These enzymes areactive from pH of 3 to 9 and at a temperature of about 100 o F. Animalderived enzymes either work in the stomach at a low pH or in theintestine at much higher pH. Since ours work over a broader range theyare active longer in the system at reducing the food into usable components.
Back to TopEnzymes; All Natural Plant Base Enzymes by Cell Tech [new window][frame][cache][preview][close preview][clusters]... CTI Enzymes contain a combination of enzymes to help break down all types of ... E-12 Super Enzymes - a superior blend of plant-based enzymes plus Cell Tech Super ...websites.celltech.com/sbgalgae01/files/enzymes.htm-Ask 1, Ask 7, MSN 17Enzyme Health [new window][frame][cache][preview][close preview][clusters]are those enzymes that are present only in raw food and contain varying quantities of the four basic types of plant enzymes: protease used in protein digestion, amylase for carbohydrate digestion, ...www.hum.org/enzyme_health.html-Wisenut 6, Ask 34, MSN 82Enzymes - plant enzymes, or food enzymes? Enzymes move our muscles ... [new window][frame][cache][preview][close preview][clusters]Plants are dependent on free enzymes in the soil to help make plant food, and suffer ... the integrity of metabolic enzymes, and abuse the enzymes' potential, we are inviting the most serious types ...www.simplecom.net/timeless/digest.htm-MSN 9, Ask 16
Alpha & Beta Amylase –3,150 DUProteases – 20,500 HUTLipase – 265 LUCellulase – 110 CUHemicellulase – 100 HCUBromelain – 20,000 FCCProbiotic (Bacillus coagulans) – 600 Million CFU
Nutritional InformationCrude Protein- 5.0% min.,Crude Fat- 0%,Crude Fiber- 0%,Moisture- 6.0% max.
Contains no lactose, sugars or preservatives. Add 1/4 teaspoon to each cup of food Plant enzymes: $10.75
Digestive enzymes are special types of protein molecules that catalyzethe breakdown of food into components that can be utilized by the body.These proteins are not stored in the body but are released based on theanticipation aroma or actual presence of food in the digestive system.Because they are not stored they must be taken with each meal,preferably with the food. Merritt's enzymes contain a blend of plant andmicrobial produced enzymes. None of them are from animal sources.
Each enzyme is highly specific as to the class of food it works on andthe temperature and pH of its effective range of activity. Animalderived enzymes will work in only one area of the digestive system,while plant and microbial enzymes work throughout the whole system, frommouth through the stomach into the intestines. As the body ages lessenzymes are produced and supplementation is necessary to assure optimumhealth.
To maintain optimum health in an animal it needs to be fed an optimum,diet, but also needs to have digestive efficiency necessary toassimilate the food ingredients. The digestive efficiency can be reducedby stress of any sort, excitement , anxiety (travel separation, workingstress and so on. To insure optimum digestion and health we recommendthe addition of this supplement to each meal. For optimum utilizationthe supplement should be added to the food and should be moistenedshortly before feeding to be effective.
Since Merritt's enzymes are derived from plant and microbial sourcesthey are active throughout the whole gastrointestinal tract not in aspecific section, as animal derived enzymes are. These enzymes areactive from pH of 3 to 9 and at a temperature of about 100 o F. Animalderived enzymes either work in the stomach at a low pH or in theintestine at much higher pH. Since ours work over a broader range theyare active longer in the system at reducing the food into usable components.
Back to TopEnzymes; All Natural Plant Base Enzymes by Cell Tech [new window][frame][cache][preview][close preview][clusters]... CTI Enzymes contain a combination of enzymes to help break down all types of ... E-12 Super Enzymes - a superior blend of plant-based enzymes plus Cell Tech Super ...websites.celltech.com/sbgalgae01/files/enzymes.htm-Ask 1, Ask 7, MSN 17Enzyme Health [new window][frame][cache][preview][close preview][clusters]are those enzymes that are present only in raw food and contain varying quantities of the four basic types of plant enzymes: protease used in protein digestion, amylase for carbohydrate digestion, ...www.hum.org/enzyme_health.html-Wisenut 6, Ask 34, MSN 82Enzymes - plant enzymes, or food enzymes? Enzymes move our muscles ... [new window][frame][cache][preview][close preview][clusters]Plants are dependent on free enzymes in the soil to help make plant food, and suffer ... the integrity of metabolic enzymes, and abuse the enzymes' potential, we are inviting the most serious types ...www.simplecom.net/timeless/digest.htm-MSN 9, Ask 16
Wednesday, March 01, 2006
Addiction Vs Dependance
Pain pills: Avoiding addiction
There's little risk of becoming addicted to prescription pain medications if you follow your doctor's directions for use.
The injury was months ago and you've done everything your doctor suggested — stretching, strengthening exercises, ice, heat — but you still hurt.
Over-the-counter pain remedies aren't helping, and you'd like to try something stronger. But you're also somewhat hesitant. What about all the celebrities who've wound up addicted to prescription pain medication? Would that happen to you?
The short answer: Probably not.
What is addiction?
Pain specialists define addiction very precisely. The key component is that an addict uses a drug compulsively, despite the fact that it causes harm. A prime example is cigarettes. Most smokers know that cigarettes damage their health. Many want to quit, but can't overcome the craving. That's addiction.
People who are, or have been, addicted to one drug are at higher risk of becoming addicted to other drugs. Addictive disorders also tend to be inherited. If you have family members who abuse drugs or alcohol, you're at higher risk of the same problem.
Addiction vs. dependence
Some people confuse addiction with physical dependence, a condition that results in withdrawal symptoms if the drug is suddenly stopped.
Many types of nonaddictive drugs — including corticosteroids and beta blockers — can cause physical dependence. These types of drugs should not be stopped abruptly. Instead, the dosage should be reduced gradually, so the person can be weaned off the medication.
Addiction and physical dependence often occur together. But you can have addiction without physical dependence, and physical dependence without addiction.
Addictive pain medications
Some of the most addictive pain medications are opioids, a family of drugs that have effects similar to those of opium or morphine.
Commonly prescribed opioids include codeine, propoxyphene (Darvon, others), meperidine (Demerol, others), hydrocodone (Vicodin, others), hydromorphone (Dilaudid, others), oxycodone (OxyContin, others) and morphine (MS Contin, others).
Who's at risk?
The vast majority of people who take their pain medication as directed never become addicted, even during long-term use. The key is to take the medication exactly as prescribed by a physician. Frequent assessment and follow-up with your doctor will ensure that you're taking the safest and most effective amount of medication.
The addiction risk is higher for people who have a family or personal history of drug or alcohol abuse. This additional risk is lessened in people participating in 12-step recovery programs such as Alcoholics Anonymous and who have family support.
Mistaken identity
People with unrelieved chronic pain sometimes act in ways that appear to be addictive. They may be preoccupied with maintaining their supply of medicine or anxiously watch the clock so that they won't miss their next dose. These behaviors, called pseudoaddiction, typically stop once the person gets satisfactory pain relief.
It also is common for people to develop a tolerance to their pain medication, needing higher doses to achieve the same level of pain relief. This is normal, and not a sign of addiction. In some cases, tolerance proves to be helpful, as many of a drug's side effects may disappear once your body becomes more used to the medicine.
Be honest with your doctor
Tell your doctor if you have had a particular side effect from a pain medication in the past. Also share your personal and family history of substance abuse or addiction. Your doctor needs this information to choose the type of pain medication that will work best for you.
***********************************************************************
Taken from the Mayo clinic website
http://www.mayoclinic.com/health/pain-pill-addiction/PN00056
***********************************************************************
There's little risk of becoming addicted to prescription pain medications if you follow your doctor's directions for use.
The injury was months ago and you've done everything your doctor suggested — stretching, strengthening exercises, ice, heat — but you still hurt.
Over-the-counter pain remedies aren't helping, and you'd like to try something stronger. But you're also somewhat hesitant. What about all the celebrities who've wound up addicted to prescription pain medication? Would that happen to you?
The short answer: Probably not.
What is addiction?
Pain specialists define addiction very precisely. The key component is that an addict uses a drug compulsively, despite the fact that it causes harm. A prime example is cigarettes. Most smokers know that cigarettes damage their health. Many want to quit, but can't overcome the craving. That's addiction.
People who are, or have been, addicted to one drug are at higher risk of becoming addicted to other drugs. Addictive disorders also tend to be inherited. If you have family members who abuse drugs or alcohol, you're at higher risk of the same problem.
Addiction vs. dependence
Some people confuse addiction with physical dependence, a condition that results in withdrawal symptoms if the drug is suddenly stopped.
Many types of nonaddictive drugs — including corticosteroids and beta blockers — can cause physical dependence. These types of drugs should not be stopped abruptly. Instead, the dosage should be reduced gradually, so the person can be weaned off the medication.
Addiction and physical dependence often occur together. But you can have addiction without physical dependence, and physical dependence without addiction.
Addictive pain medications
Some of the most addictive pain medications are opioids, a family of drugs that have effects similar to those of opium or morphine.
Commonly prescribed opioids include codeine, propoxyphene (Darvon, others), meperidine (Demerol, others), hydrocodone (Vicodin, others), hydromorphone (Dilaudid, others), oxycodone (OxyContin, others) and morphine (MS Contin, others).
Who's at risk?
The vast majority of people who take their pain medication as directed never become addicted, even during long-term use. The key is to take the medication exactly as prescribed by a physician. Frequent assessment and follow-up with your doctor will ensure that you're taking the safest and most effective amount of medication.
The addiction risk is higher for people who have a family or personal history of drug or alcohol abuse. This additional risk is lessened in people participating in 12-step recovery programs such as Alcoholics Anonymous and who have family support.
Mistaken identity
People with unrelieved chronic pain sometimes act in ways that appear to be addictive. They may be preoccupied with maintaining their supply of medicine or anxiously watch the clock so that they won't miss their next dose. These behaviors, called pseudoaddiction, typically stop once the person gets satisfactory pain relief.
It also is common for people to develop a tolerance to their pain medication, needing higher doses to achieve the same level of pain relief. This is normal, and not a sign of addiction. In some cases, tolerance proves to be helpful, as many of a drug's side effects may disappear once your body becomes more used to the medicine.
Be honest with your doctor
Tell your doctor if you have had a particular side effect from a pain medication in the past. Also share your personal and family history of substance abuse or addiction. Your doctor needs this information to choose the type of pain medication that will work best for you.
***********************************************************************
Taken from the Mayo clinic website
http://www.mayoclinic.com/health/pain-pill-addiction/PN00056
***********************************************************************
Wednesday, February 22, 2006
Nausea Help
This will be an ongoing post to which I will add more information as it comes to hand. If there is something you wish to add please use “comments” and I will add it to the body of the post. These idea’s are not intended to replace any nausea treatment you are now receiving. These idea’s were posted on the PMB.
Robin H
“Zofran, 4 mg. by IV, is by far the best for me for nausea”
“classic (not diet!) Coca-Cola, at room temperature (cold will induce vomiting) and take a teaspoon at a time “
saltine crackers
CJ
mint tea
ginger tea
ginger ale soda7 up
crackersphenerganZofranKytrilCompazine,
Raglan
Inap
Levisin sublingual
Rhonda
Compazine
Jennifer
Phenergan
Zofran
Cindy
Reglan
Brett
Maxalon
Mint tea
Boiled candy
Ginger ale (ginger Soda) Must have real ginger in it
Ice cube held between joint of thumb and index finger
Pete
Saltine crackers(no salt)
Ginger Ale
Phenergran 25mg
flat Coke-room temp
Robin H
“Zofran, 4 mg. by IV, is by far the best for me for nausea”
“classic (not diet!) Coca-Cola, at room temperature (cold will induce vomiting) and take a teaspoon at a time “
saltine crackers
CJ
mint tea
ginger tea
ginger ale soda7 up
crackersphenerganZofranKytrilCompazine,
Raglan
Inap
Levisin sublingual
Rhonda
Compazine
Jennifer
Phenergan
Zofran
Cindy
Reglan
Brett
Maxalon
Mint tea
Boiled candy
Ginger ale (ginger Soda) Must have real ginger in it
Ice cube held between joint of thumb and index finger
Pete
Saltine crackers(no salt)
Ginger Ale
Phenergran 25mg
flat Coke-room temp
Subscribe to:
Posts (Atom)